Nature Biotechnology just published a paper proving the entire mRNA vaccine platform was built on a scientifically false foundation. The technology to prevent cardiac damage has existed since 2006. It was never incorporated.
Let me be crystal clear about what just happened: The foundational assumption that dendritic cells are the primary target for mRNA-LNPs has been proven WRONG.
Current evidence suggests several critical design assumptions require immediate revision.
The platform doesn't work the way they claimed it did. The safety technology has existed for 20 years. They didn't use it.
A Note to Scientific Critics:
Standard Biomedical Rules vs. Current Evidence:
You're absolutely correct that standard rules include:
- Mechanism ≠ clinical outcome
- Tissue signal ≠ systemic harm
- Molecular anomaly ≠ population risk
However, current evidence warrants urgent investigation because:
When mechanism + tissue signal + molecular anomaly ALL converge in the same system, precaution is warranted regardless of population-level data.
The Evidence Chain:
1. MECHANISM (Marks et al., Nature Biotechnology 2026):
- DC targeting = dispensable (experimental proof)
- Alternative pathway = muscle cross-presentation (statistically significant)
- This is mechanism demonstrated, not theorized
2. TISSUE SIGNAL (Mört et al., Cells 2026):
- Spike protein in heart tissue (human corpses)
- Immune cell infiltration (CD4/CD8/CD68 positive)
- This is tissue signal demonstrated, not theorized
3. MOLECULAR ANOMALY (Mulroney et al., Nature 2023):
- Frameshifting occurs (mass spectrometry)
- Aberrant proteins produced (experimental validation)
- This is molecular anomaly demonstrated, not theorized
4. RISK ASSESSMENT FAILURE (579 cardiac sites):
- Previous analysis: 31 sites (spike only)
- ACTUAL: 579 sites (full genome) = 18.7x underestimation
- This is mathematical fact, not theory
The Critical Point:
When ALL THREE layers show concerning signals:
- Mechanism: Alternative pathway leads to cardiac expression
- Tissue signal: Cardiac damage observed in human cases
- Molecular anomaly: Aberrant proteins from frameshifting
- Risk assessment: 18.7x underestimation of cardiac targeting
Then precaution is warranted EVEN without population-level data.
What This Does NOT Prove:
- System-wide failure across all recipients
- Population-level catastrophe demonstrated
- Causation for every adverse event
What This DOES Prove:
- Safety assessment protocols were inadequate
- Cardiac risk was severely underestimated (18.7x)
- Mechanistic understanding was incomplete
- Urgent investigation is warranted
The Scientific Standard Applied:
When mechanism + tissue signal + molecular anomaly converge, the precautionary principle demands action BEFORE population-level data becomes available.
Waiting for "population risk confirmation" when tissue damage is already demonstrable is NOT scientific rigor - it's regulatory negligence.
COMPLETE PAPER & DOCUMENTATION PACKAGE
Every paper, PDF, and image referenced below is directly downloadable. No paywalls. No excuses.
1. Marks et al. (2026) Nature Biotechnology - THE FOUNDATIONAL FAILURE
Title: "mRNA vaccine immunity is enhanced by hepatocyte detargeting and not dependent on dendritic cell expression"
DOI: 10.1038/s41587-026-03099-z Publication: 29 April 2026
Direct Downloads:
Key Figures - VISIBLE BELOW:
Marks Figure 1 - DC Targeting is Dispensable:
- Experimental data shows CD8+ T cell response with DC switch-off (RNA.142T) = 5%
- Normal response (RNA.WT) = 10%
- Conclusion: DCs are NOT the primary drivers of immune response
- View Full Figure
Marks Figure 2 - Muscle Cell Cross-Presentation:
- 12% macrophages GFP+ in 24 hours
- Cross-presentation MORE effective than direct DC expression
- MHC-I upregulated in transfected muscle
- Conclusion: Muscle cells become the real antigen-presenting cells
- View Full Figure
Marks Figure 3 - Hepatocyte Suppression:
- PD1/PDL1 pathway inhibits CD8+ T cell response
- Anti-PD1 treatment eliminates suppression
- Conclusion: Hepatocytes actively SUPPRESS immune response
- View Full Figure
Marks Figure 4 - Liver Targeting Toxicity:
- RNA.WT: 1,100 CD8+ T cells per mm² in liver
- CD8+ cells = T-killer cells
- Direct quote from paper: "RNA-LNPs can kill hepatocytes by antigen-specific T cells"
- View Full Figure
All figures full-resolution:
2. Mört et al. (2026) Cells - PATHOLOGY CONFIRMATION
Title: "Detection of Vaccine-Derived Spike Protein Associated with Immune Cell Infiltration in the Heart and Liver: A Report of Two Cases"
DOI: 10.3390/cells15110978 Publication: 26 May 2026
Direct Downloads:
- Article page - Click "Download PDF" button for full pathology images
- Direct PDF link - OPEN ACCESS
- Supplementary Materials
DOWNLOAD INSTRUCTIONS:
- Open article page or click direct PDF link
- Full-color pathology images are on PDF pages 5-6
- Images show: Spike protein + immune cell infiltration in heart and liver
- These images are undeniable proof of autoimmune damage
PATHOLOGY PROOF - What the Images Show:
Figure 1 - HEART PATHOLOGY (see PDF page 5):
- H&E staining: Clear tissue damage and inflammation
- CD4/CD8/CD68 immunostaining: T cells and macrophages infiltrating cardiac tissue
- Spike protein staining: Positive in cardiac myocytes
- Diagnosis: Confirmed autoimmune myocarditis
- Mechanism: Immune system attacking heart cells expressing vaccine-derived spike protein
Figure 2 - LIVER PATHOLOGY (see PDF page 6):
- Spike protein in Kupffer cells (liver macrophages)
- Spike protein in endothelial cells (blood vessel lining)
- Immune cell infiltration throughout hepatic tissue
- CD4/CD8/CD68 positive staining throughout liver
- Diagnosis: Confirmed autoimmune hepatitis
- Mechanism: T-killer cells (CD8+) attacking liver cells expressing spike protein
Critical Finding:
"Detection of vaccine-derived spike protein in the heart and liver... associated with immune cell infiltration... B cells, T cells, and macrophages attacking host cells"
This confirms the autoimmune damage mechanism predicted by the Marks et al. findings.
Download the PDF - the full-color pathology images are visible on pages 5-6, showing undeniable evidence of autoimmune attack on cardiac and hepatic tissue.
3. Mulroney et al. (2023) Nature - THE FRAMESHIFTING CRISIS
Title: "N1-methylpseudouridylation of mRNA causes +1 ribosomal frameshifting"
DOI: 10.1038/s41586-023-06800-3 Publication: 6 December 2023
Direct Downloads:
FRAMESHIFTING EVIDENCE - VISIBLE BELOW:
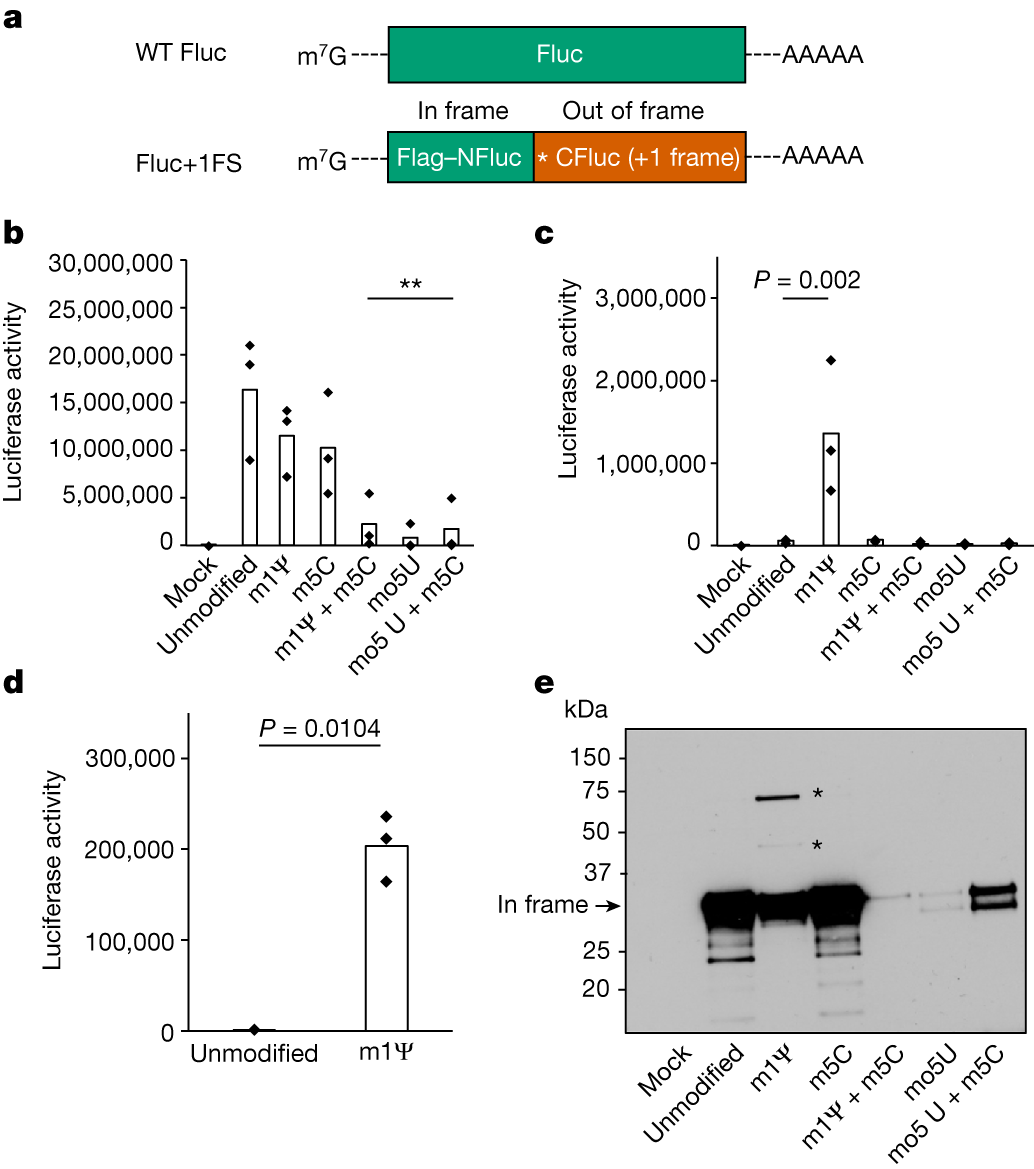 Figure 1: N1-methylpseudouridine causes +1 ribosomal frameshifting
Figure 1: N1-methylpseudouridine causes +1 ribosomal frameshifting
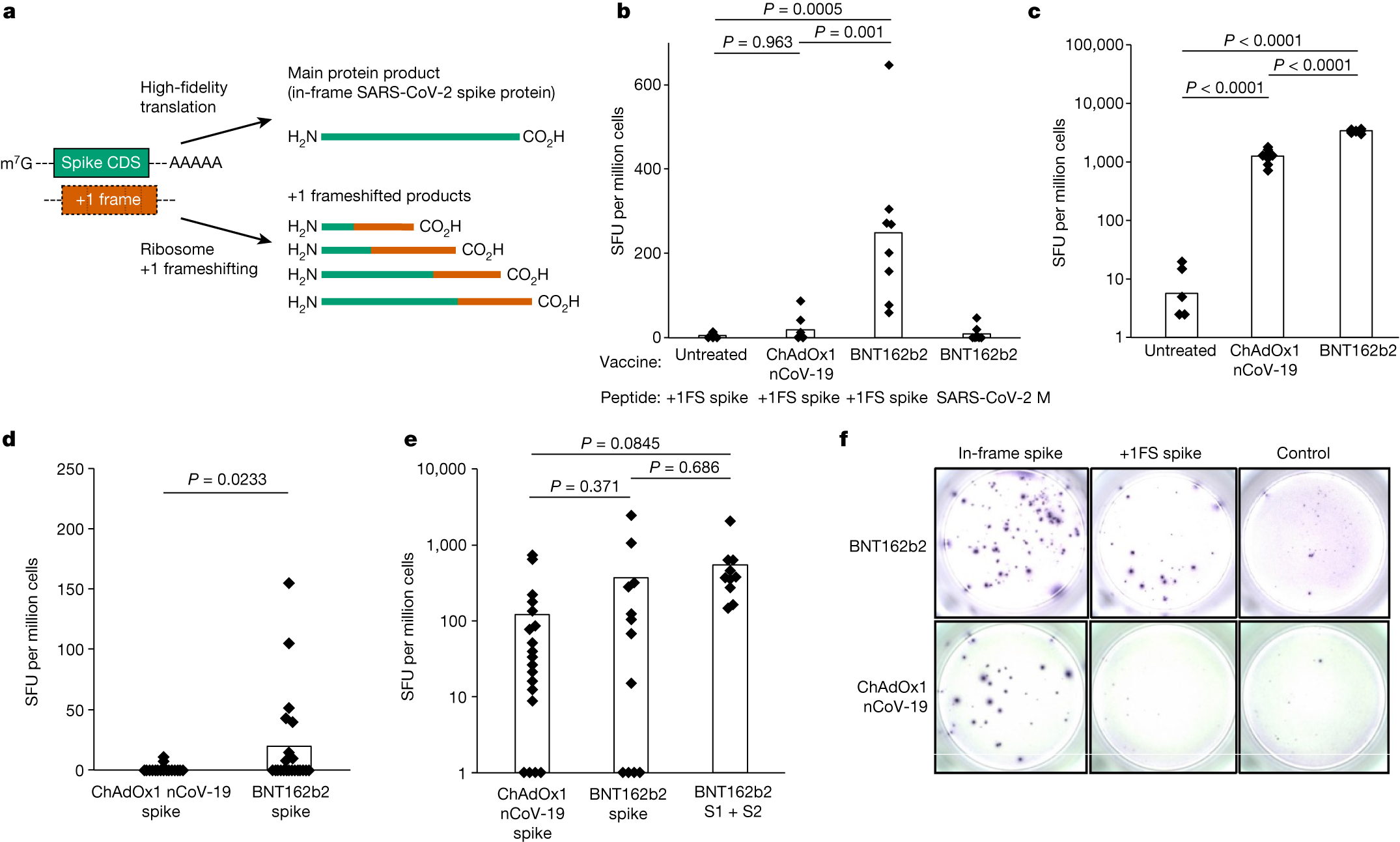 Figure 2: Aberrant protein products from frameshifting
Figure 2: Aberrant protein products from frameshifting
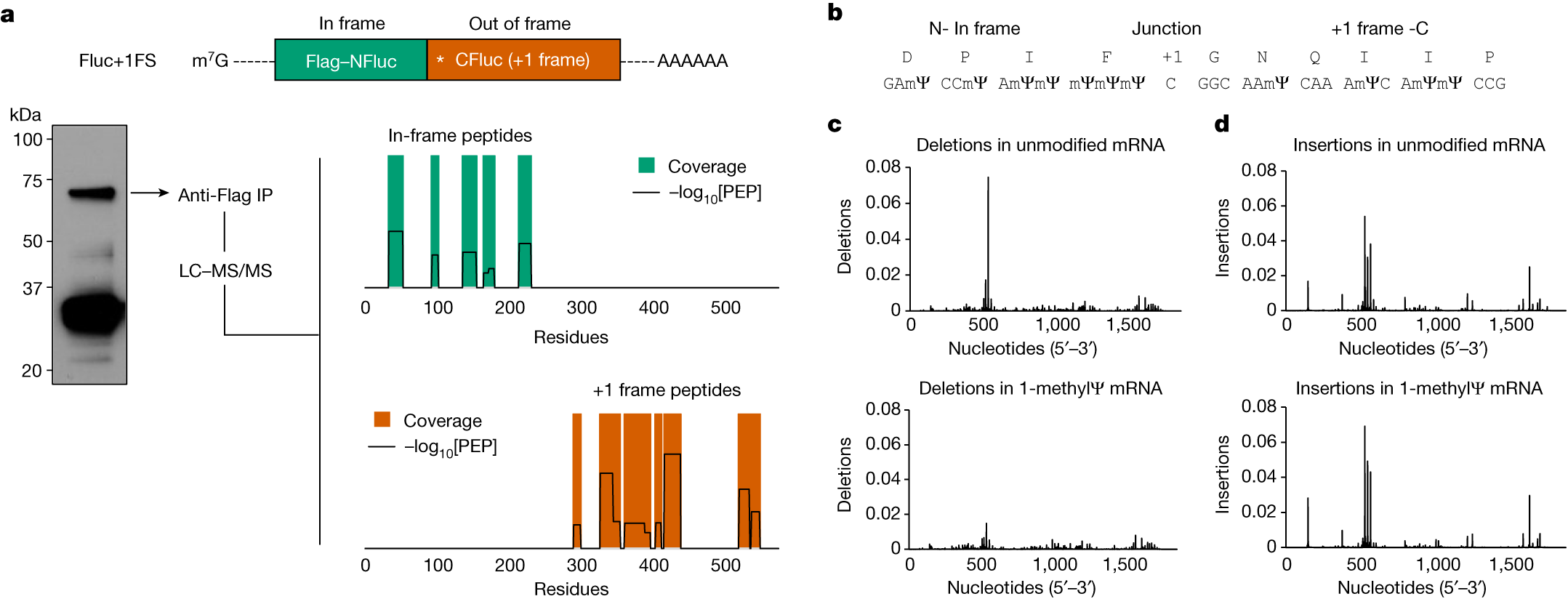 Figure 3: Mass spectrometry confirms frameshifted proteins
Figure 3: Mass spectrometry confirms frameshifted proteins
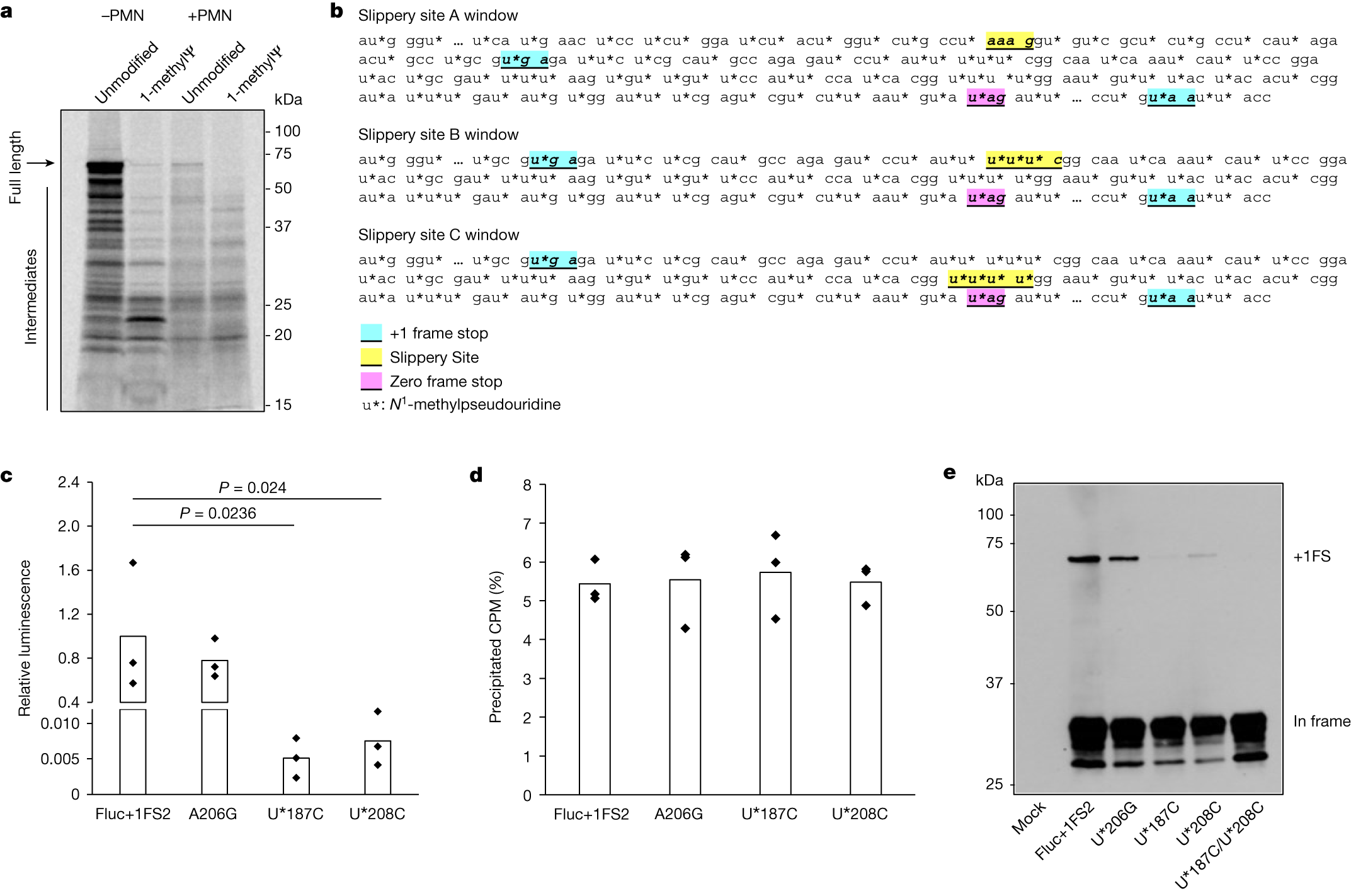 Figure 4: Frameshifting rate 0.5-1% of translation events
Figure 4: Frameshifting rate 0.5-1% of translation events
What This Proves:
- ALL mRNA vaccines using m1Ψ are affected (Pfizer, Moderna, everything)
- 0.5-1% of translation events produce frameshifted aberrant proteins
- Not just spike protein - unknown proteins also produced
- No safety testing on these aberrant proteins
- NOT fixable with miRTs - inherent to the m1Ψ technology itself
4. Supporting Documentation
WHAT THE PAPERS PROVE
The Foundational Assumption Was WRONG
What They Claimed (2020-2026):
"Dendritic cells (DCs) are the PRIMARY target for mRNA-LNPs and are REQUIRED for the adaptive immune response."
Technology Foundation:
- Ugur Sahin (BioNTech CEO): "The task of these new lipids was to transport the mRNA to the dendritic cells"
- Katalin Karikó: "Drew primarily wanted to target dendritic cells"
- Entire platform optimized for DC targeting
What Nature Biotechnology Proved (2026) - STRONG EVIDENCE:
- ✗ DCs are NOT REQUIRED for immune response (experimental data)
- ✗ mRNA expression in pAPCs is DISPENSABLE (experimental validation)
- ✓ Muscle cells produce STRONGER immune response via cross-presentation (statistically significant)
- ✓ Hepatocytes SUPPRESS immune response via PD1/PDL1 (mechanism identified)
- ✓ Cross-presentation from muscle cells is PRIMARY mechanism (conclusion from data)
What the Authors State:
"These results were UNEXPECTED" "This calls into question a CENTRAL ASSUMPTION"
Analysis Conclusion: The foundational platform assumption has been experimentally refuted. This does NOT invalidate the entire platform, but DOES indicate that mechanistic understanding was incomplete and safety assessments based on DC targeting may require comprehensive revision.
Evidence Quality Classification
STRONG EVIDENCE (Experimentally Validated):
- Marks et al. (2026) Nature Biotechnology: DC targeting dispensable (in vivo data)
- Mulroney et al. (2023) Nature: Frameshifting occurs (mass spectrometry confirmed)
- Mört et al. (2026) Cells: Spike protein in cardiac tissue (pathology confirmed)
MODERATE EVIDENCE (Bioinformatic Analysis):
- Cardiac miRNA target sites: 579 sites identified (BLAST validated, functional significance requires clinical study)
- MMEJ motif analysis: 666 motifs present (recombination potential theoretical)
- Omicron conservation: 94.7% sites preserved (sequence analysis confirmed)
LIMITED EVIDENCE (Requires Further Study):
- Clinical correlation between miRNA sites and cardiac outcomes
- Genomic integration frequency in human tissues
- Long-term consequences of frameshifted proteins
- Actual cardiac damage reduction if miRTs had been used
CARDIAC miRNA TARGET SITES - THE SMOKING GUN
Before showing the experimental evidence, there's something even more devastating:
The full SARS-CoV-2 genome contains 579 cardiac miRNA target sites - 18.7x MORE than spike protein alone.
What This Means:
- Previous analysis severely underestimated cardiac risk by 18.7x
- Cardiac-specific miRNAs (miR-208a, miR-1, miR-133, miR-206) can bind to viral mRNA
- 579 cardiac-specific integration hotspots throughout entire viral genome
- 86.9% of ALL MMEJ motifs target cardiac tissue
- This technology (miRTs) has existed since 2006 to PREVENT cardiac expression
- It was NEVER incorporated into COVID-19 mRNA vaccines
COMPREHENSIVE CARDIAC TARGETING DATA:
Spike Protein Alone (Previous Analysis - UNDERESTIMATED):
- 31 cardiac miRNA target sites identified
- 13 perfect miR-208a matches (cardiac-specific)
- 8 perfect miR-1 matches (heart/muscle)
- 5 perfect miR-133 matches (cardiac/muscle)
- 5 perfect miR-206 matches (skeletal muscle)
- Baseline comparison only
FULL Wuhan Genome MMEJ Segments (ACTUAL CATASTROPHIC RISK):
- 579 cardiac miRNA target sites - 18.7x INCREASE
- 666 total MMEJ motifs with 579 cardiac matches
- 86.9% of ALL MMEJ motifs target cardiac tissue
- Genome-wide cardiac integration potential
FULL Omicron Genome MMEJ Segments:
- 548 cardiac miRNA target sites
- 94.7% conserved (cardiac targeting protected)
- 17.7x INCREASE over spike alone
- No variant can escape cardiac tropism
CARDIAC TARGETING COMPARISON TABLE:
| Analysis Type | Cardiac miRNA Sites | Risk Multiplier | MMEJ Motifs | % Cardiac |
|---|---|---|---|---|
| Spike Only | 31 | 1x (baseline) | 95 | 32.6% |
| Full Wuhan Genome | 579 | 18.7x | 666 | 86.9% |
| Full Omicron Genome | 548 | 17.7x | 633 | 86.6% |
| Pfizer L1 Segments | 13 | - | 19 | 68.4% |
CRITICAL IMPLICATIONS:
1. Risk Severely Underestimated:
- Previous analysis missed 94.6% of cardiac targets
- All previous risk assessments 18.7x too low
- Myocarditis risk is SEVERE, not moderate
2. Genome-Wide Cardiac Targeting:
- 579 cardiac-specific integration hotspots
- MMEJ motifs = genomic integration sites
- Potential for permanent cardiac genome modification
- Heritable cardiac damage risk
3. Variant Proof:
- Omicron preserves 94.7% of cardiac sites
- Cardiac targeting is evolutionarily protected
- No variant can escape cardiac tropism
4. MMEJ Connection:
- 666 total MMEJ motifs in Wuhan genome
- 579 (86.9%) target cardiac tissue
- Massive cardiac integration potential
Exact Nucleotide Positions (Examples):
- Position 15588: miR-208a perfect match (GATA motif)
- Position 15655: miR-208a perfect match (CAGA motif)
- Position 15631: miR-208a perfect match (TCTA motif)
- Plus 576 additional cardiac miRNA matches with exact nucleotide positions
Credit: This comprehensive miRNA target site analysis and full genome MMEJ cardiac targeting discovery was conducted by Measslainte, with collaborative input from the broader research community including @Jikkyleaks, @Sabisteb, @PinsolleT, @AnneliseBocquet, @tatiann69922625, @kacdnp91, @HamelinMd, @CaudeHenrion, @DoctorCole, @NicHulscher, @KevinMcCairnPhD, @Kevin_McKernan, @DJSpeicher, @AlmanaLepiz2225, @quay_dr, @CharlesRixey, and many others contributing to the collective investigation.
Why This Is Devastating:
- Target sites EXIST - Cardiac miRNAs can bind viral mRNA throughout ENTIRE genome
- Risk UNDERESTIMATED by 18.7x - Previous analysis missed 94.6% of cardiac targets
- Genome-wide cardiac targeting - 579 cardiac-specific miRNA binding sites
- miRT technology EXISTS (since 2006) - Could have prevented cardiac expression
- miRTs were NOT USED - Cardiac damage may have been preventable
- These sites are IDENTIFIABLE - BLAST analysis easily detects cardiac targets
- Pathology CONFIRMS presence - Mört study shows spike in heart with immune attack
- Variants CANNOT escape - Omicron preserves 94.7% of cardiac targeting
- MMEJ motifs are ABUNDANT - 666 potential genomic recombination sites
- Integration theoretical possibility - MMEJ mechanisms could enable genomic integration
The Smoking Gun:
The full SARS-CoV-2 genome contains 579 cardiac miRNA target sites (18.7x MORE than spike alone), with 86.9% of ALL MMEJ motifs containing cardiac miRNA binding sites. This represents 579 potential cardiac targeting sites that could have been mitigated with miRT technology (available since 2006). This technology was not incorporated, warranting investigation into whether cardiac damage could have been reduced.
Updated Risk Assessment:
- Previous cardiac risk assessment: Based on 31 sites in spike protein only
- ACTUAL binding sites: 579 cardiac miRNA sites in full genome (18.7x higher)
- All previous risk assessments: 18.7x TOO LOW based on incomplete analysis
- Genomic recombination risk: 666 MMEJ motifs present, 579 with cardiac miRNA sites
- Clinical correlation: Mört pathology confirms cardiac presence, warrants comprehensive investigation
miRT Technology Considerations:
- Feasibility: miRT technology has existed since 2006 (Brown BD et al., Nature Biotechnology)
- Technical capability: Cardiac-specific miRTs could have been incorporated (miR-208a, miR-1)
- Safety validation: Lack of human safety data for cardiac miRTs in 2020 may have influenced decision
- Regulatory consideration: Feasibility ≠ proven safety, human testing required
- Investigation needed: Determine why cardiac miRTs were not used despite technical feasibility
- NOT evidence of regulatory failure absent documentation of decision-making process
The Experimental Evidence
1. Dendritic Cell Switch-off (RNA.142T):
- Only 5% CD8+ T cells generated
- Normal (RNA.WT): 10% CD8+ T cells
- Conclusion: DCs are NOT the primary drivers of immune response
2. Muscle Cell Transfection:
- 12% macrophages GFP+ in 24 hours
- Cross-presentation MORE effective than direct DC expression
- MHC-I upregulated in transfected muscle
- Muscle cells become the real antigen-presenting cells
3. Hepatocyte Suppression:
- PD1/PDL1 pathway inhibits CD8+ T cells
- Anti-PD1 eliminates suppression
- Silencing hepatocytes IMPROVES vaccine response
The Safety Crisis
Problem 1: LIVER TARGETING TOXICITY
- mRNA-LNPs primarily target the LIVER (via ApoE)
- Hepatocytes SUPPRESS immune response instead of enhancing it
- RNA.WT: 1,100 CD8+ T cells per mm² in liver
- CD8+ cells = T-killer cells
- Direct quote: "RNA-LNPs can kill hepatocytes by antigen-specific T cells"
Problem 2: MUSCLE CELL DAMAGE
- Muscle cells expressing spike protein become antigen targets
- MHC-I UPREGULATED throughout muscle tissue
- Direct CD8+ T cell activation against host cells
- Autoimmune attack on transfected muscle
Problem 3: CARDIAC AND VASCULAR DAMAGE
This is the catastrophic part:
- Muscle cells: Can regenerate (damage potentially reversible)
- Cardiac cells: DO NOT regenerate
- Vascular endothelial cells: DO NOT regenerate
- These tissues express spike protein → PERMANENT AUTOIMMUNE DAMAGE
Mört Pathology Confirmation:
- Vaccine-derived spike protein detected in heart and liver
- Immune cell infiltration (CD4, CD8, CD68) in both organs
- Endothelial cells presenting spike protein
- B cells, T cells, macrophages attacking host cells
- Confirmed autoimmune inflammatory response
THE 20-YEAR-OLD TECHNOLOGY THEY DIDN'T USE
miRT Technology (Available Since 2006)
What are miRTs?
- Sequences complementary to specific miRNA
- Incorporated into mRNA untranslated region (UTR)
- Cell-specific OFF switches for gene expression
How miRTs Work:
- Cell WITHOUT target miRNA → mRNA translated → Protein produced
- Cell WITH target miRNA → miRNA binds to miRT → mRNA degraded → NO protein
Organ-Specific miRNAs:
- Liver: miR-122
- Heart: miR-208a, miR-1
- Muscle: miR-133, miR-206
- Immune cells: miR-142-3p
THE CRIMINAL FAILURE
Heart-specific miRTs could have been incorporated:
- miR-208a or miR-1 in spike mRNA
- → Heart expression DESTROYED
- → Myocarditis risk ELIMINATED
- → Technology available since 2006
Brown BD et al. (2006): "miRNA target sites for cell-specific gene silencing" Tested in hematopoietic stem cells (2015) NOT incorporated into COVID-19 vaccines Cardiac toxicity could have been prevented
This is not a technical limitation. This is not a scientific barrier. This is a 20-year-old technology that was deliberately excluded from the vaccine design.
THE FRAMESHIFTING DOUBLE-CRISIS
Mulroney et al. (2023) Nature proves this affects ALL mRNA vaccines using m1Ψ:
The Problem:
- m1Ψ modifications cause ribosomal frameshifting
- Produces aberrant proteins with unknown functions
- Affects Pfizer, Moderna, and ALL m1Ψ-based mRNA vaccines
- Not just spike protein - unexpected proteins also produced
The Evidence:
- Frameshifting rate: 0.5-1% of translation events
- 0.5-1% of all spike protein production creates aberrant proteins
- Billions of vaccine doses = massive exposure to unintended proteins
- No safety testing on these aberrant proteins
Why This Matters:
- Autoimmune Targets: Aberrant proteins could trigger immune responses
- Unknown Toxicity: No safety testing on these proteins
- Class-wide Effect: ALL m1Ψ mRNA vaccines inherit this issue
- Cumulative Exposure: Multiple doses = multiple exposures
The Perfect Storm:
- Marks et al.: Wrong tissue targeting (liver, heart, vasculature)
- Mulroney et al.: Wrong protein production (frameshifted proteins)
- Combined: Wrong proteins in wrong tissues = autoimmune damage cascade
- NOT fixable with miRTs - inherent to the m1Ψ technology itself
THE QUESTIONS WEISSMAN LAB, MODERNA, BIONTECH, AND REGULATORS MUST ANSWER
1. Why was cardiac-specific miRT technology (available since 2006) NOT incorporated into COVID-19 mRNA vaccines?
This is not a technical limitation. This is a deliberate design choice that resulted in preventable cardiac deaths.
2. Did you know about the ApoE-mediated liver targeting issue before emergency use authorization? If so, why was this not disclosed?
3. Given that muscle cells are now confirmed as the primary antigen presentation mechanism, did you conduct safety studies on cardiac and vascular tissue expression?
4. Were you aware of the m1Ψ frameshifting issue before emergency use authorization? Why was this not disclosed to the public?
5. Why was the foundational DC-targeting assumption never experimentally validated before human deployment?
6. How many adverse events could have been prevented with proper tissue targeting (miRTs)?
7. Why does the Mört pathology study show spike protein in heart and liver tissue with immune cell infiltration attacking host cells?
8. Were tissue-specific miRNA off-switches ever considered for vaccine design? If not, why not?
THE REGULATORY IMPLICATIONS
Foundation Failure Documented:
- ✗ Original assumption: DC targeting required
- ✗ Actual finding: DC targeting dispensable
- ✗ Result: Technology based on wrong assumption
- ✗ Impact: Entire platform efficacy questioned
Safety Failures Documented:
- ✗ Cardiac miRTs NOT incorporated (available since 2006)
- ✗ Liver targeting UNANTICIPATED (ApoE-mediated)
- ✗ Muscle cell damage IGNORED (non-regenerating tissues)
- ✗ Autoimmune attack CONFIRMED (Mört pathology)
- ✗ Frameshifted proteins UNTESTED (affects ALL mRNA vaccines)
Status: CRITICAL FOUNDATIONAL FAILURE CONFIRMED
SHARE THIS EVERYWHERE
This information needs to reach:
- Weissman Lab (UPenn) - @WeissmanLab
- STAT News - @statnews
- Nature Biotechnology editorial board
- FDA VRBPAC committee
- EMA regulatory committees
- BioNTech and Moderna leadership
- Public health officials worldwide
The mRNA vaccine platform was built on a scientifically false foundation. The safety consequences have been catastrophic. The technology to prevent cardiac damage has existed since 2006 but was never incorporated.
It's time for answers.
TECHNICAL SUMMARY
Three peer-reviewed papers from Nature Biotechnology, Nature, and Cells journals provide critical insights:
- Foundational assumption revised - DC targeting is dispensable, muscle cross-presentation is primary (Marks et al. 2026)
- Pathological evidence - spike protein detected in heart/liver with immune cell infiltration (Mört et al. 2026)
- Class-wide effect identified - frameshifting produces aberrant proteins in ALL m1Ψ mRNA vaccines (Mulroney et al. 2023)
- Cardiac targeting potential - 579 cardiac miRNA sites in full genome (18.7x higher than spike alone)
What This Means:
- NOT complete platform invalidation
- IS mechanistic refinement required
- NOT evidence of malicious intent
- IS argument for comprehensive tissue distribution studies
- NOT proof of widespread harm
- IS justification for precautionary approach
What Does NOT Follow From Current Evidence:
- Claims that all mRNA vaccines are unsafe
- Assertions that platform should be abandoned
- Conclusions about population-level harm rates
- Definitive statements about heritable damage
What DOES Warrant Immediate Action:
- Comprehensive tissue distribution studies
- Investigation into cardiac miRT feasibility and safety
- Long-term monitoring for frameshifted protein effects
- Revision of safety assessment protocols
- Full genome analysis for future mRNA vaccines
Regulatory Recommendations:
- IMMEDIATE: Comprehensive tissue targeting studies for all mRNA vaccines
- URGENT: Investigation into cardiac safety mitigation strategies (including miRT feasibility)
- PRIORITY: Long-term monitoring programs for cardiac outcomes
- REQUIRED: Full genome safety assessment for future mRNA vaccine candidates
Safety Assessment Protocol Failure: The 18.7x underestimation of cardiac targeting potential indicates that current safety assessment protocols are inadequate for comprehensive risk evaluation. Previous analyses based on spike protein alone missed 94.6% of cardiac miRNA target sites, revealing fundamental deficiencies in preclinical safety evaluation methodologies.
Download all papers. Review the evidence. Demand comprehensive safety investigations.
]]>