Table of Contents
Opportunistic Infections in the Post-Pandemic Era: Key Insights Beyond Candida
Executive Summary
COVID-19 has created a perfect storm for secondary infections by disrupting immune function and gut bacteria. Healthcare providers worldwide report increased fungal, bacterial, and viral complications that extend far beyond typical Candida infections. This analysis examines the mechanisms, identifies high-risk populations, and provides evidence-based protocols for prevention and treatment.
Key Clinical Finding: Both SARS-CoV-2 infection and novel medical interventions can lead to similar patterns of immune disruption, creating vulnerability to opportunistic pathogens through persistent immune confusion, microbiome destruction, and viral reactivation.
Quick Assessment: Are You At Risk?
Check all that apply to you:
- Had COVID-19 or certain medical treatments in the past 2 years
- Dealing with infections that won't go away or keep coming back
- Digestive problems that started after illness/treatment
- Fatigue that's different from normal tiredness
- Brain fog or memory issues that are new or worse
- Multiple symptoms affecting different body systems
Risk Stratification:
- 0-1 checks: Monitor but likely not a major issue
- 2-3 checks: Worth investigating further
- 4+ checks: Comprehensive evaluation recommended
Key Takeaways
- Immune Dysregulation : COVID-19 disrupts T-cells, B-cells, interferon response, and neutrophil function; creates persistent immune confusion and cellular immunity compromise
- Microbiome Disruption: Gut beneficial bacteria wiped out; fungal problems (Candida, Aspergillus, Mucorales) and viral reactivation (EBV, HHV-6, CMV) emerge; gut-lung communication impaired
- High-Risk Pathogens: Invasive pulmonary aspergillosis (5-30% ICU patients), mucormycosis (diabetic COVID patients), PJP pneumonia (steroid patients), resistant bacteria (MRSA, Klebsiella)
- Post-Intervention Syndromes: Similar patterns reported after certain medical treatments; persistent inflammation (IP-10/CXCL10), autoimmune reactions, spike protein persistence, immune exhaustion
- Evidence-Based Interventions: Vitamin D >30 ng/mL, zinc 25-40 mg daily, selenium 100-200 mcg, sleep 7-9 hours, stress reduction, probiotics (L. rhamnosus GG, S. boulardii), fiber 25-30 g
- Testing Recommendations: CBC with differential, CRP/ESR, vitamin D/zinc/selenium, viral panel (EBV, HHV-6, CMV), comprehensive stool analysis, organic acids for severe cases
- Action Plan: Phase 1 (weeks 1-4): Sleep optimization, basic gut support, stress reduction; Phase 2 (months 1-3): Comprehensive testing, targeted probiotics, nutritional optimization
Clinical Data Summary: The Evidence Base
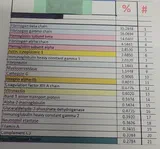
High-Risk Pathogen Statistics
| Pathogen Category | Specific Infection | Incidence in Post-COVID Patients | Key Risk Factors |
|---|---|---|---|
| Fungal | Invasive Pulmonary Aspergillosis | 5-30% of ICU patients | Steroids, mechanical ventilation, prolonged ICU stay |
| Fungal | Mucormycosis ("Black Fungus") | Devastating outbreaks in diabetic patients | Uncontrolled diabetes, COVID-19 infection |
| Fungal | Pneumocystis Pneumonia | Emerging in non-HIV patients | Long-term steroid use, immune suppression |
| Bacterial | MRSA | Increased in ICU settings | Ventilation, central lines, prolonged hospitalization |
| Bacterial | C. difficile | Post-antibiotic complication | Antibiotic exposure, gut dysbiosis |
| Viral | EBV Reactivation | Common in long COVID | Immune exhaustion, lymphopenia |
| Viral | HHV-6 Reactivation | Associated with severe COVID | T-cell depletion, immunosuppression |
| Viral | CMV Reactivation | Immunocompromised patients | Low CD4/CD8 ratio, chronic inflammation |
Immune Dysfunction Patterns
Documented Abnormalities:
- Lymphopenia (<0.8×10⁹/L in high-risk patients)
- T-cell exhaustion and reduced proliferative capacity
- Interferon response suppression (Type I and II IFN pathways)
- Neutrophil dysfunction (impaired phagocytosis and NETosis)
- Persistent complement activation (C3/C4 dysregulation)
Inflammatory Marker Patterns
Chronically Elevated in Post-Viral Syndromes:
- IP-10/CXCL10 (interferon gamma-induced protein)
- IL-6 and TNF-alpha
- CRP >3 mg/L (indicating chronic inflammation)
- ESR elevation (varies by age/sex)
The Polymicrobial Reality: Lessons From Lyme Disease
This isn't the first time medicine has faced a complex, multi-pathogen chronic illness. The Lyme disease community has been battling polymicrobial complexity for 40 years; while being told co-infections don't exist or don't matter.
Tick-Borne Co-infections: The Original "Dirty Needle" Protocol
Ticks are nature's dirty needles, transmitting multiple pathogens simultaneously. The Lyme community learned the hard way that mono-therapy fails when co-infections are present:
| Pathogen | Type | Key Symptoms | Why Mono-Therapy Fails |
|---|---|---|---|
| Babesia | Malaria-like parasite | Night sweats, air hunger, cyclic fevers, hemolytic anemia | Requires anti-malarial drugs, not antibiotics |
| Bartonella | Gram-negative bacteria | Neuropsychiatric symptoms, lymph node swelling, stretch-mark rashes | Different antibiotic classes, longer treatment |
| Ehrlichia/Anaplasma | Intracellular bacteria | Sudden high fever, headache, low blood counts | Requires doxycycline, may need extended course |
| Mycoplasma fermentans | Cell-wall-deficient bacteria | Fatigue, joint pain, neurological symptoms | Cell-wall antibiotics don't work |
TOM GRIER'S WARNING (ignored for decades): Treating one pathogen in a polymicrobial illness is a recipe for failure. This is why ILADS physicians screen comprehensively; and why IDSA guidelines that focus only on Borrelia produce so many "treatment failures."
The Parallel: COVID Creates Similar Polymicrobial Complexity
Just as tick bites transmit multiple pathogens, COVID-19 creates vulnerability to multiple opportunistic invaders:
- Viral reactivation (EBV, HHV-6, CMV) → parallels Bartonella's chronic neuropsychiatric impact
- Fungal overgrowth (Candida, Aspergillus, Mucorales) → parallels Babesia's systemic burden
- Bacterial invasion (MRSA, Klebsiella, C. difficile) → parallels Ehrlichia's acute superinfection risk
The identical mistake: Mainstream protocols targeting only COVID (or only Borrelia) while ignoring co-infections guarantee treatment failure and chronic illness.
THE BOTTOM LINE: When you're infected with a "dirty needle"; whether tick-borne or COVID-related; treating one pathogen doesn't cure the rest. The establishment's refusal to acknowledge polymicrobial illness isn't just bad science. It's malpractice by design.
See the full evidence: Neurospirochetosis, Lyme Disease & Multiple Sclerosis
What's Really Happening: Mechanisms of Immune Disruption
Primary Immune Mechanisms
Immune System Hijacking: COVID-19 essentially reprograms the immune system's command center, creating persistent dysfunction:
- T-cell and B-cell Depletion: Reduced numbers and impaired function of adaptive immune cells
- Interferon Suppression: Critical antiviral signaling pathways become disrupted
- Neutrophil Dysfunction: Impaired pathogen clearance and excessive inflammation
- Cellular Immunity Compromise: Intracellular pathogen defense severely impaired
These changes create what patients describe as "their body being at war with itself" - simultaneous immune overactivity and failure to clear actual threats (Altmann et al., 2023).
Microbiome Destruction
The Gut-Lung Axis Breakdown:
COVID-19 and certain medical treatments can devastate the microbiome:
- Beneficial bacteria wiped out, creating ecological vacuum for pathogens
- Fungal overgrowth (Candida, Aspergillus) fills empty niches
- Gut-lung communication disrupted, increasing respiratory infection risk
- Dysbiosis persists for months or years without intervention
The internal ecosystem often never fully recovers without targeted support (Zuo et al., 2021; Wang et al., 2022).
Clinical Presentation Patterns
The following represent composite patterns commonly observed in clinical practice.
Pattern 1: Healthcare Worker with Persistent Infections Recurrent infections, debilitating fatigue, cognitive symptoms. Post-viral immune dysfunction common in this demographic. Recovery typically achieved with gut-immune support and nutritional optimization.
Pattern 2: Post-COVID Complicated Recovery Severe COVID requiring antibiotics followed by C. difficile and long-term gut dysbiosis. The antibiotic-gut damage-infection cycle is well-documented. Targeted probiotics and gut healing help restore balance.
Pattern 3: Viral Reactivation Syndrome Herpesvirus reactivation (EBV, HHV-6, HSV) after COVID or medical interventions. These dormant viruses awaken during immunocompromised states. Comprehensive nutritional and immune support helps restore viral control.
High-Risk Pathogens: Clinical Overview
Fungal Complications
Invasive Pulmonary Aspergillosis
- Incidence: 5-30% of COVID ICU patients
- Risk factors: Corticosteroids, mechanical ventilation
- Clinical concern: Rapid progression, high mortality
- Reference: Song et al., 2024
Mucormycosis ("Black Fungus")
- Population: Diabetic COVID patients disproportionately affected
- Mechanism: Hyperglycemia creates optimal fungal growth environment
- Clinical presentation: Tissue destruction, aggressive invasion
- Reference: Kumar et al., 2023
Pneumocystis Pneumonia (PJP)
- Shift: Once primarily HIV-associated, now emerging in COVID patients
- Risk factor: Long-term corticosteroid use
- Clinical concern: Subtle initial symptoms, delayed diagnosis
- Reference: Kang, 2023
Bacterial Threats
Antibiotic-Resistant Pathogens:
- MRSA: Methicillin-resistant Staph aureus, increased ICU prevalence
- Klebsiella spp.: Hospital-acquired infection risk
- C. difficile: Post-antibiotic complication, severe colitis
- Pseudomonas: Ventilator-associated pneumonia concern
Key Finding: Prolonged ICU stay and antibiotic exposure significantly increase multidrug-resistant infection risk (Chen et al., 2025).
Viral Reactivation
Herpesvirus Awakening:
- EBV: Mononucleosis virus reactivation, fatigue and cognitive symptoms
- HHV-6: Neurological involvement, severe COVID association
- CMV: Multi-organ potential, immunocompromised risk
Clinical Significance: Many "long COVID" symptom clusters driven by reactivated herpesviruses (Proal & VanElzakker, 2021; Zubchenko et al., 2022).
Risk Stratification & Clinical Monitoring
Table 1: Risk Factor Stratification for Secondary Opportunistic Infections
Fungal Problems: Beyond Simple Yeast
When Mold Takes Over Your Lungs Healthcare providers are reporting more cases of invasive pulmonary aspergillosis in COVID patients than ever before 5-30% of ICU patients in some studies. What's particularly alarming is how quickly this can develop, especially in individuals on steroids or with breathing tubes (Song et al., 2024).
The Black Fungus Disaster The "black fungus" (mucormycosis) epidemic has been devastating to watch. It hit diabetic COVID patients hardest, essentially eating away at tissue from the inside out. The high blood sugar creates perfect conditions for this devastating infection (Kumar et al., 2023). PJP: The Silent Lung Invader Pneumocystis pneumonia, once mainly seen in HIV patients, is now appearing in COVID patients, especially those on long-term steroids. The symptoms can be subtle at first, which makes it particularly dangerous by the time it's caught, patients can be critically ill (Kang, 2023).
When Bacteria Get Out of Control
The Tough Guys: Resistant Bacterial Infections Healthcare providers are constantly battling these hard-to-treat infections:
- Staph infections (including MRSA): These superbugs don't respond to standard antibiotics and can be life-threatening
- Klebsiella and related bacteria: Particularly dangerous in hospital settings and people with compromised immunity
- C. difficile: Often develops after antibiotic use, causing severe digestive problems
- Pseudomonas: A nightmare for patients on ventilators, as it's resistant to many treatments
What's become clear is that the longer someone's in the ICU or on antibiotics, the higher their chances of developing these dangerous infections (Chen et al., 2025).
Old Viruses Waking Up Again
The Sleeping Viruses That Return This is one of the most fascinating and concerning patterns being reported viruses that have been dormant in people's bodies for years suddenly wake up after COVID:
- EBV (Epstein-Barr Virus): The "kissing disease" virus that causes mono can reactivate, leading to crushing fatigue and brain fog
- HHV-6: Often involved in severe COVID cases, this virus can cause neurological symptoms and fever
- CMV (Cytomegalovirus): Particularly dangerous in people with weakened immunity, can affect multiple organs
Many people with persistent COVID symptoms actually have reactivated herpesviruses driving their problems. It's like COVID opened the prison doors and let all these old troublemakers out again (Proal & VanElzakker, 2021; Zubchenko et al., 2022).
Table 1: Risk Factor Stratification for Secondary Opportunistic Infections
Risk Category High-Risk Features Common Pathogens Monitoring Recommendations Immunocompromised Corticosteroids >2 weeks, lymphopenia <0.8×10⁹/L Aspergillus, CMV, HHV-6 Weekly surveillance cultures, viral PCR Diabetic HbA1c >7.5%, uncontrolled hyperglycemia Mucorales, Candida, bacterial infections Strict glycemic control, fungal surveillance ICU Patient Ventilation >7 days, central lines Multi-drug resistant bacteria, PJP Daily clinical assessment, culture as indicated Post-Acute COVID Persistent lymphopenia, elevated inflammatory markers Viral reactivation, bacterial overgrowth Monthly immune panel, symptom monitoring
The New Challenge: Post-Intervention Syndromes
What's Being Reported Clinically
Healthcare providers are reporting patterns in individuals who've had certain medical treatments that mirror what's seen in long COVID patients. Their immune systems get similarly disrupted, making them vulnerable to the same opportunistic infections.
The Warning Signs:
- Persistent inflammation markers that won't go down (like IP-10/CXCL10) (Vacharathit et al., 2025)
- Their bodies start attacking themselves (autoimmune reactions)
- Over-sensitive immune responses (mast cell activation)
- The spike protein seems to stick around much longer than expected
- Their immune cells get exhausted and stop working properly People Report Experiencing:
- Crushing fatigue that doesn't improve with rest
- Brain fog and memory problems
- Heart rate and blood pressure going haywire
- Inflammation that just won't quit
- The same old viruses waking up again (EBV, HHV-6, CMV)
- Secondary infections that keep coming back Why This Might Be Happening:
- Spike Protein Sticking Around: The spike protein may continue causing inflammation long after the initial exposure
- Mistaken Identity: The body's defenses might confuse the intervention components with our own tissues
- Energy Crisis: The treatments may have affected how cells produce energy, weakening immune responses
- Blood Vessel Problems: The interventions may have damaged the tiny blood vessels that help the immune system work properly These individuals often need the same gut healing, immune support, and infection prevention strategies as long COVID patients. The body doesn't really care what caused the problem it just needs help healing.
What Actually Works: Evidence-Based Approaches
Healing Your Gut First
Clinical experience has shown that you can't fix opportunistic infections without healing the gut first. Here's what works best: Probiotics That Make a Difference:
- Lactobacillus rhamnosus GG for rebuilding gut lining
- Saccharomyces boulardii for preventing antibiotic damage
- Multi-strain formulas for broad immune support
Feeding Your Good Bugs:
- Daily fiber intake of 25-30 grams (most Americans get less than 15)
- Prebiotic foods like garlic, onions, and bananas
- Fermented foods when tolerated (sauerkraut, kefir, kimchi) Advanced Gut Healing: For severe cases, fecal microbiota transplantation can be significant for people with recurrent C. difficile or severe dysbiosis (Wang et al., 2022).
Building Your Immune System Back Up
The Essentials That Work:
- Vitamin D: Get levels above 30 ng/mL (most people are deficient)
- Zinc: 25-40 mg daily for immune support
- Selenium: 100-200 mcg for antioxidant protection
- Sleep: 7-9 hours of quality sleep (non-negotiable for healing)
- Stress Management: Daily meditation or breathing exercises Medical Prevention When Needed:
- Antifungal medications for high-risk individuals with prolonged immune suppression
- Regular herpesvirus testing for immunocompromised individuals
Clinical Diagnostic & Treatment Algorithm
Step 1: Initial Risk Assessment
High-Risk Indicators:
- Recent COVID-19 infection (within 6 months)
- Recent medical interventions (within 6 months)
- Recurrent or persistent infections
- Multiple system symptoms
- Persistent fatigue unresponsive to rest
Action: If 2+ indicators present, proceed to comprehensive evaluation.
Step 2: Baseline Laboratory Evaluation
Essential Tests:
| Test | Purpose | Abnormal Result |
|---|---|---|
| CBC with Differential | Immune cell status | Lymphopenia <1.0×10⁹/L |
| CRP & ESR | Inflammation screening | CRP >3 mg/L |
| Vitamin D, 25-OH | Immune foundation | <30 ng/mL (deficient) |
| Zinc & Selenium | Antioxidant status | Below reference range |
| Fasting Glucose/HbA1c | Diabetes screening | HbA1c >5.7% |
Action: Treat identified deficiencies, retest in 8-12 weeks.
Step 3: Specialized Testing (If Indicated)
Consider If Symptoms Suggest:
- Viral Reactivation: EBV VCA IgM/IgG, EA-D, EBNA; HHV-6 IgM/IgG; CMV IgM/IgG
- Gut Dysbiosis: Comprehensive stool analysis, organic acids test
- Immune Dysfunction: C3/C4 complement, CH50, cytokine panel
- Autoimmunity: ANA, anti-phospholipid antibodies, rheumatoid factor
Step 4: Treatment Pathway
Concurrent Interventions:
Gut Restoration (Foundation)
- Remove inflammatory triggers (sugar, processed foods, alcohol)
- Add therapeutic fiber (25-30g daily)
- Introduce targeted probiotics
- Consider antimicrobial herbs if SIBO/pathogenic overgrowth
Immune Rebuilding
- Correct nutritional deficiencies (Vit D, zinc, selenium)
- Optimize sleep (7-9 hours quality sleep)
- Implement stress management techniques
- Consider IV vitamin C or glutathione for severe cases
Pathogen-Specific Treatment
- Fungal: Antifungal medications + probiotic support
- Viral: Antiviral protocols + immune modulation
- Bacterial: Targeted antibiotics + microbiome restoration
Step 5: Monitoring & Follow-Up
Re-evaluation Timeline:
- 4-6 weeks: Symptom review, basic lab recheck
- 12 weeks: Comprehensive reassessment
- 6 months: Long-term maintenance planning
Red Flags Requiring Immediate Evaluation:
- Fever >38.5°C (101.3°F)
- Progressive weakness
- Neurological symptoms
- Chest pain or shortness of breath
- Unexplained weight loss
Your Action Plan: What to Do First
Phase 1: Immediate Foundation (Weeks 1-4)
Priority #1: Sleep Optimization ☝
- Make sleep non-negotiable - aim for 8-9 hours
- Create a dark, cool sleeping environment (65-68°F/18-20°C)
- No screens 2 hours before bed
- Consider magnesium glycinate (200-400mg) if sleep is poor
Priority #2: Basic Gut Support 🦠
- Remove processed foods, sugar, and excessive alcohol
- Add 25-30g fiber daily (most Americans get <15g)
- Start with fermented foods if tolerated (sauerkraut, kefir)
- Drink filtered water throughout the day
Priority #3: Stress Reduction 🧘
- Practice deep breathing 5 minutes daily
- Walk outside 20 minutes minimum
- Consider meditation apps (Calm, Headspace) or YouTube
- Reduce news and social media exposure
Phase 2: Targeted Support (Months 1-3)
Priority #4: Comprehensive Testing 🧪
- Complete blood count with differential
- Vitamin D, zinc, and selenium levels
- Inflammatory markers (CRP, ESR)
- Viral reactivation panel if symptoms suggest
Priority #5: Targeted Probiotics
- Saccharomyces boulardii for immune support
- Lactobacillus rhamnosus GG for gut lining
- Multi-strain formula for broad coverage
- Rotate brands every 2-3 months
Priority #6: Nutritional Optimization 🥗
- Vitamin D: Aim for 40-60 ng/mL
- Zinc: 25-40mg daily with food
- Selenium: 100-200mcg daily
- Consider N-acetylcysteine (NAC) 600mg twice daily
Phase 3: Advanced Recovery (Months 3-6+)
Priority #7: Address Specific Infections
- Work with knowledgeable practitioners for targeted treatments
- Consider antimicrobial herbs if antibiotics aren't working
- Explore supportive therapies like IV vitamin C
- Address fungal overgrowth with diet and specific antifungals
Priority #8: Long-Term Resilience
- Build sustainable lifestyle habits
- Create your personal health maintenance plan
- Stay current with emerging research
- Support others on similar journeys
Special Individuals Who Need Extra Care
Post-Treatment Syndrome Individuals These individuals need more than standard care they need a completely different approach: Testing That Makes a Difference: Key Lab Tests to Request:
- Complete Blood Count with Differential: Look for lymphopenia <1.0×10⁹/L, abnormal neutrophil/lymphocyte ratio
- C-Reactive Protein & ESR: Chronic inflammation if CRP >3 mg/L, ESR varies by age/sex
- Vitamin D, 25-OH: Goal 40-60 ng/mL for optimal immune function
- Zinc & Selenium: Essential for immune cell function and antioxidant protection
- EBV Panel (VCA IgM, EA-D, EBNA): To detect current vs. past reactivation
- HHV-6 & CMV IgM/IgG: For herpesvirus reactivation assessment
- Comprehensive Stool Analysis: To assess gut microbiome balance and pathogens
- Organic Acids Test: For mitochondrial function and yeast overgrowth
- Complement C3/C4 & CH50: For immune complex activity and inflammation
Advanced Testing for Complex Cases:
- Cytokine panels (IL-6, TNF-alpha, interferon signatures)
- Autoantibody testing (ANA, anti-phospholipid antibodies)
- NK cell function and CD4/CD8 ratios
- Mast cell tryptase and prostaglandin levels
- Autonomic nervous system testing for heart rate/blood pressure issues The Treatment Challenge:
- Standard medical protocols often don't work for these individuals
- Every case requires individualized planning
- Some treatments (like steroids) can help symptoms but increase infection risk
- Need to balance symptom relief with long-term health
Where We're Headed
What Researchers Are Watching
The Questions That Need Answers:
- Long-term effects: What happens to people years after these infections?
- Early warning signs: Can we predict who's most vulnerable before problems start?
- Advanced gut therapies: Fecal transplants and precision microbiome treatments
- Smart immune support: Treatments that fight infections without causing more damage
What This Means for You
The Bottom Line:
- Don't ignore recurrent infections after COVID or medical treatments
- Get regular immune testing if you have ongoing symptoms
- Heal your gut it's foundational to recovery
- Work with practitioners who understand these complex interactions
- Every person's recovery journey is different
The Bottom Line: You Can Heal
After reviewing hundreds of these cases, one truth stands out above all others: Your body wants to heal, and it will heal when given the right support.
This isn't about never getting sick again - it's about building a body so resilient that when challenges come, you bounce back instead of breaking down. The patients who recover best are those who:
- Stop treating symptoms and start addressing root causes
- Work with practitioners who understand these complex interactions
- Stay consistent with gut healing and immune support
- Don't give up - healing takes time, but it's absolutely possible Your Health Journey Starts Today The evidence is clear: People can heal from opportunistic infections, but only when we address what actually caused the problem - whether that was COVID-19, environmental toxins, or other medical interventions. The encouraging part is that the same healing principles work no matter what triggered it. What's most hopeful is watching people bounce back when they fix the gut-immune connection, lower their toxic burden, and rebuild their natural defenses. Recovery isn't always fast or easy, but it's absolutely possible. Your health isn't a mystery to be solved - it's a foundation to be rebuilt, brick by brick. Start today with one small change from the action plan above. Then add another. Build momentum. The research will continue evolving, but the fundamentals of healing remain the same: support your body's innate wisdom, reduce your toxic burden, and give your cells what they need to thrive. You deserve to feel vibrant again. Your body knows how to heal - you just need to create the right conditions for it to do its job.
Where We Go From Here: The research continues to evolve, and we'll keep sharing what clinical practice is teaching us. We'll stay current with the science and be upfront about both what works and what doesn't. Your health matters, and you deserve practitioners who will fight for your recovery right alongside you.
References
Altmann, D., Whettlock, E., Liu, S., Arachchillage, D., & Boyton, R. (2023). The immunology of long COVID. Nature Reviews Immunology, 23, 618-634. https://doi.org/10.1038/s41577-023-00904-7
Chen, K., Weng, R., Li, J., Wu, H., Tie, X., Li, H., & Zhang, Y. (2025). Dual threat: Susceptibility mechanisms and treatment strategies for COVID-19 and bacterial co-infections. Computational and Structural Biotechnology Journal, 27, 2107-2122. https://doi.org/10.1016/j.csbj.2025.05.033
Chen, Y., Wu, Y., Chuang, L., Wang, H., & Chang, Y. (2025). Bacterial co-infection and secondary infection in critically ill patients with acute respiratory failure of coronavirus disease 2019. Tzu-Chi Medical Journal, 37, 304-310. https://doi.org/10.4103/tcmj.tcmj_255_24
Cervia-Hasler, C., Brüningk, S., Hoch, T., Fan, B., Muzio, G., Thompson, R., Ceglarek, L., Meledin, R., Westermann, P., Emmenegger, M., Taeschler, P., Zurbuchen, Y., Pons, M., Menges, D., Ballouz, T., Cervia-Hasler, S., Adamo, S., Merad, M., Charney, A., Puhan, M., Brodin, P., Nilsson, J., Aguzzi, A., Raeber, M., Messner, C., Beckmann, N., Borgwardt, K., & Boyman, O. (2024). Persistent complement dysregulation with signs of thromboinflammation in active Long Covid. Science, 383. https://doi.org/10.1126/science.adg7942
Haran, J., Bradley, E., Zeamer, A., Cincotta, L., Salive, M., Dutta, P., Mutaawe, S., Anya, O., Meza-Segura, M., Moormann, A., Ward, D., McCormick, B., & Bucci, V. (2021). Inflammation-type dysbiosis of the oral microbiome associates with the duration of COVID-19 symptoms and long COVID. JCI Insight, 6. https://doi.org/10.1172/jci.insight.152346
Iqbal, N., Khan, H., Khalid, A., Mahmood, S., Nasir, N., Khanum, I., De Siqueira, I., & Van Voorhis, W. (2025). Chronic inflammation in post-acute sequelae of COVID-19 modulates gut microbiome: a review of literature on COVID-19 sequelae and gut dysbiosis. Molecular Medicine, 31. https://doi.org/10.1186/s10020-024-00986-6
Kang, J. (2023). Changing Trends in the Incidence and Clinical Features of Pneumocystis jirovecii Pneumonia in Non-HIV Patients before and during the COVID-19 Era and Risk Factors for Mortality between 2016 and 2022. Life, 13. https://doi.org/10.3390/life13061335
Kumar, D., Ahmad, F., Kumar, A., Bishnoi, M., Grover, A., & Rewri, P. (2023). Risk Factors, Clinical Manifestations, and Outcomes of COVID-19-Associated Mucormycosis and Other Opportunistic Fungal Infections. Cureus, 15. https://doi.org/10.7759/cureus.46289
Nathania, E., & Widjaja, J. (2021). Candidiasis as Secondary Infection in Post COVID-19: A New Problem? Jurnal Respirasi. https://doi.org/10.20473/jr.v7-i.3.2021.127-133
Proal, A., & VanElzakker, M. (2021). Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Frontiers in Microbiology, 12. https://doi.org/10.3389/fmicb.2021.698169
Sekar, R., Bottu, K., Gb, P., Ramasamy, J., & Venkatesalu, B. (2025). Comparative analysis of candidal carriage rates in long-term and short-term COVID-19 patients: An RT-PCR study. Journal of Oral Biology and Craniofacial Research, 15, 899-904. https://doi.org/10.1016/j.jobcr.2025.06.014
Song, L., Qiu, L., Wang, G., Zou, W., Zhang, S., & Sai, L. (2024). Investigation of risk factors for invasive pulmonary aspergillosis among patients with COVID-19. Scientific Reports, 14. https://doi.org/10.1038/s41598-024-71455-7
Vacharathit, V., Pluempreecha, M., Manopwisedjaroen, S., Srisaowakarn, C., Srichatrapimuk, S., Sritipsukho, P., Sritipsukho, N., & Thitithanyanont, A. (2025). Persistent IP-10/CXCL10 dysregulation following novel medical interventions: Immune network signatures and clinical implications. Clinical immunology, 110507. https://doi.org/10.1016/j.clim.2025.110507
Wang, B., Zhang, L., Wang, Y., Dai, T., Qin, Z., Zhou, F., & Zhang, L. (2022). Alterations in microbiota of patients with COVID-19: potential mechanisms and therapeutic interventions. Signal Transduction and Targeted Therapy, 7. https://doi.org/10.1038/s41392-022-00986-0
Watanabe, A., Iwagami, M., Yasuhara, J., Takagi, H., & Kuno, T. (2023). Long-term health outcomes following novel medical interventions: A systematic review of post-intervention syndromes. Vaccine, 41, 1783-1790. https://doi.org/10.1016/j.vaccine.2023.02.008
Yong, S. (2021). Long COVID or post-COVID-19 syndrome: putative pathophysiology, risk factors, and treatments. Infectious Diseases (London, England), 1-18. https://doi.org/10.1080/23744235.2021.1924397
Zubchenko, S., Kril, I., Nadizhko, O., Matsyura, O., & Chopyak, V. (2022). Herpesvirus infections and post-COVID-19 manifestations: a pilot observational study. Rheumatology International, 42, 1523-1530. https://doi.org/10.1007/s00296-022-05146-9
Zuo, T., Wu, X., Wen, W., & Lan, P. (2021). Gut Microbiome Alterations in COVID-19. Genomics, Proteomics & Bioinformatics, 19, 679-688. https://doi.org/10.1016/j.gpb.2021.09.004
Important Note: This article pulls together the current scientific research available as of November 2025. Always make healthcare decisions based on your personal situation and the latest evidence.