Table of Contents
Key Takeaways
- Neurospirochetosis Evidence : Autopsy series from 1911 to present describe living Borrelia burgdorferi spirochetes in brains of deceased MS patients across at least 10 countries
- Testing Limitations: Standard Lyme testing plagued by false negatives due to strain variability, immune response differences, and rigid diagnostic criteria; "negative" result does not rule out infection
- Beyond Ticks: Transmission may extend beyond ticks to other arthropods (fleas, mites, lice, bed bugs) and bodily fluids (semen, blood, urine, saliva); sexual/contact transmission biologically plausible
- Alzheimer's Connection: Borrelia burgdorferi found in ~25% of Alzheimer's cases (far more than controls); periodontal Treponemas observed in >90% of AD brains
- Inflammatory Food Triggers: Gluten (zonulin → leaky gut), A1 dairy (BCM-7 → gut/brain inflammation), legumes (lectins/phytates), nightshades, and industrial seed oils feed inflammation
- Antimutagenic Support: Cruciferous vegetables (sulforaphane), green tea (EGCG), red grapes/blueberries (resveratrol), onions/capers (quercetin), and fiber provide genome defense
- Family Clustering: Likely due to shared exposure (same house, pests, pets, water) and genetic propensity affecting ability to clear infections
Start here
If you look, you find it. For over a century, pathologists have reported spirochetes in brains, then we pretended not to see them. Lyme's agent, Borrelia burgdorferi, doesn't stop at joints; it crosses endothelium, enters the CNS, and leaves footprints that overlap MS. Tests miss it. Gatekeepers dismiss it. Patients live it.
What this gives you:
- What autopsies and stains actually show about Borrelia in brains
- Why "negative" tests don't mean nothing's there
- How transmission likely extends beyond ticks
- What you can do now: remove food triggers, stack antimutagens, and track your response
Neurospirochetosis & MS
MS may be linked to spirochetes, specifically Borrelia burgdorferi sensu lato, the bacterium behind Lyme disease. Across at least ten countries and more than a century of reports, autopsy series (1911 → present) describe living Lyme spirochetes in the brains of deceased MS patients. Meanwhile, standard testing in living patients is plagued by false negatives, and many still test positive for active Lyme.
Receipts that keep getting erased:
- Living Borrelia detected in MS brains.
- Borrelia burgdorferi found in ~25% of Alzheimer's cases, far more than in controls.
- Periodontal Treponemas observed in >90% of Alzheimer's brains.
The thread through it all: neurospirochetosis is visible when you actually look.
Evidence for a Conspiracy of Silence
You don't have to take my word for it. Forensic pathology work has documented:
"Microscopic images of cystic spirochetes are difficult to ignore… endowments have nearly expunged all cystic spirochetal image data from current textbooks… Variously sized cystic spirochetal profiles within diseased nerve cells explain: Lewy bodies, Pick bodies, ALS spherical bodies, Alzheimer plaques… spirochetes are hiding in plain sight."
https://doi.org/10.1016/j.mehy.2006.02.035
Why The Establishment Can Claim "It's Cured" (When It Isn't)
The official narrative depends on a simple lie: that Borrelia is an easy target for antibiotics. It isn't. The bacterium has survived for millions of years because it's a persistence specialist, and the medical establishment has spent decades pretending this basic biological fact doesn't exist.
The Persistence Playbook: How Borrelia Hides in Plain Sight
Research documented that spirochetes were found in brains. The work proved those spirochetes shouldn't even be alive after standard antibiotic treatment. Here's the survival toolkit the IDSA guidelines pretend doesn't exist:
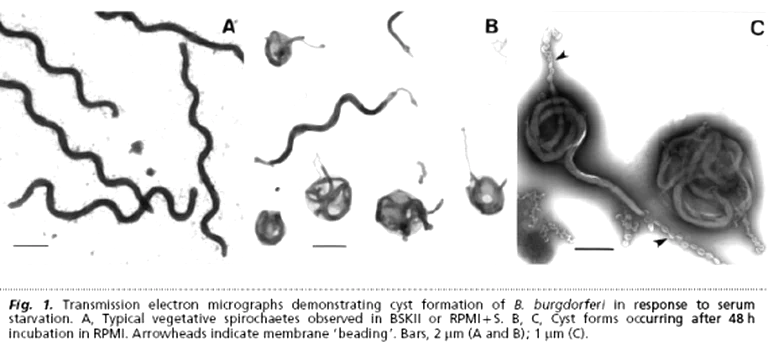
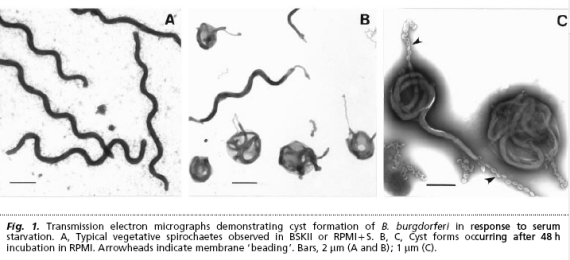
Round Body/Cyst Forms (The Dormant Enemy) When Borrelia faces pressure (antibiotics, pH shifts, temperature changes), it doesn't die. It shape-shifts into dormant round bodies (cysts) that antibiotics can't touch. These forms can survive for months, then revert back to motile spirochetes when conditions improve. The cyst in your cover image? That's not a dying bacterium. That's a bunker.
HISTORICAL RED FLAG: Cystic spirochete images were systematically erased from textbooks. The visual evidence was literally removed from medical education; once you've seen the cyst form, you can't unsee why doxy fails.
Biofilm Communities (The Fortress) Eva Sapi's 2012 study proved Borrelia forms protective biofilm-like aggregates encased in a matrix. These structures:
- Block antibiotic penetration
- Shield bacteria from immune detection
- Allow gradual re-seeding of infection
Intracellular Hiding (The Trojan Horse) Fibroblasts. Endothelial cells. Neural cells. Borrelia invades them all without killing the host cell. From inside, it's protected from both antibodies and most antibiotics. This is why the pathogen can persist for decades in tissues, while blood tests come back "negative."
Persister Cells (The Zombie State) A subpopulation enters slow-growing dormancy, highly tolerant to antibiotics that target active metabolism. Zhang's Johns Hopkins lab proved these persister cells survive standard Lyme antibiotics better than actively dividing spirochetes.
THE BOTTOM LINE: Standard treatment regimens were designed for actively dividing spirochetes. They were never tested against round bodies, biofilms, or intracellular reservoirs. The "cure" statistics are based on a rigged game.
Pleomorphic survival forms of B. burgdorferi: motile spirochete, dormant round body (cyst), and protective biofilm aggregate. Standard antibiotics target only the first form.
The Rash That Wasn't There: Built-In Diagnostic Failure
The "bull's-eye" erythema migrans (EM) rash is the diagnostic hallmark, or so we're told. Here's the reality the CDC doesn't emphasize:
- Bull's-eye pattern = minority (~20–30% of cases)
- Most EM rashes are solid red, expanding without central clearing
- 20–30% of confirmed cases have no recalled rash at all
- Common misdiagnoses: spider bite, cellulitis, ringworm, allergic reaction
This isn't an unfortunate coincidence. When your "hallmark sign" is absent in most cases, diagnostic failure is baked into the system. By the time the rash disappears or never appears, the bacteria have already disseminated. The testing window closes before most patients even seek care.
ENGINEERED DENIAL: The IDSA's insistence on bull's-eye confirmation creates a perfect diagnostic trap. No bull's-eye = no Lyme = no treatment = persistent infection = "must be something else."
Lyme vs MS
Microbiologists have documented that MS isn't a standalone disease; Lyme can drive the syndrome. The evidence shows why the establishment plugs its ears.
Highlights:
- Mother-to-child transmission of Borrelia across the womb
- B. burgdorferi + B. miyamotoi with amyloid plaques in AD brains
- Borrelia in Lewy body dementia
- Nematode worms reported in CSF of MS patients
- Borrelia signals in glioblastoma multiforme
- B. mayonii and B. burgdorferi found in human testicles
- Borreliosis is a family, not one bug/one symptom, B. miyamotoi sits alongside B. burgdorferi in brains → eradicate together
Download: MS and Lyme research summary (PDF)
Testing: why "negative" isn't negative
Lyme testing misses people.
- Strain variability: narrow antigen panels ignore the rest.
- Immune variability: not everyone mounts textbook antibodies.
- Gatekeeping: rigid criteria write patients off while labs/insurers save face.
Result: misdiagnosis, delay, damage, while the infection marches on.
When Standard Testing Fails: Diagnostic Alternatives
The standard two-tier serology (ELISA + Western blot) is designed for surveillance, not diagnosis. Here's what frontline clinicians actually use when standard testing comes up empty:
Advanced Testing Options:
| Method | What It Detects | Strength | Limitation |
|---|---|---|---|
| Culture | Live bacteria | Gold standard proof | Low sensitivity, weeks-long incubation |
| PCR | Bacterial DNA | High specificity | Poor sensitivity in blood/CSF for late disease |
| LTT/MELISA | T-cell response | Detects active infection | Limited availability, insurance coverage |
| Nanotrap antigen | Bacterial proteins (e.g., OspA) | Direct detection | Emerging technology, validation ongoing |
THE SYSTEM TRAP: By the time antibodies appear (weeks post-infection), Borrelia has already invaded protected niches. Early testing = false negative. Late testing = may miss dormant forms. Either way, the system wins, you lose.
CRITICAL DISTINCTION: CDC surveillance criteria are for epidemiological tracking, not individual patient care. Using surveillance case definitions as diagnostic gatekeeping is like using census data to decide whether an individual person exists.
Transmission: the map is bigger than ticks
Ticks (Ixodes spp.) are the primary vector, but the story doesn't end there.
- Other arthropods: bed bugs, fleas, mites, lice have been implicated to varying degrees.
- Bodily fluids: Borrelia DNA/organisms detected in semen, blood, urine, saliva, yes, that puts sexual/contact transmission on the table.
Why it clusters in families
- Genetic propensity: some people struggle to clear infections.
- Shared exposure: same house, same pests, same pets, same water, same risk.
Human-to-human?
Lyme is treatable with antibiotics, and there's no sign of casual person-to-person spread during treatment.
Ticks Are Dirty Needles: The Co-Infection Reality
Lyme disease is rarely a solo act. Ticks transmit multiple pathogens simultaneously; Borrelia is just the opening act*.
Common Co-Infections (What Else Is Hiding)
| Pathogen | Type | Key Symptoms | Treatment |
|---|---|---|---|
| Babesia | Malaria-like parasite | Night sweats, air hunger, cyclic fevers, hemolytic anemia | Anti-malarial drugs |
| Bartonella | Gram-negative bacteria | Neuropsychiatric symptoms, lymph node swelling, stretch-mark rashes | Different antibiotics |
| Ehrlichia/Anaplasma | Intracellular bacteria | Sudden high fever, headache, low blood counts, elevated liver enzymes | Doxycycline |
| Mycoplasma fermentans | Cell-wall-deficient bacteria | Fatigue, joint pain, neurological symptoms | Combination therapy |
Why this matters: Mono-therapy targeting only Borrelia often fails because:
- Different pathogens require different drugs
- Co-infections suppress immune function, enabling Borrelia persistence
- Symptoms overlap, masking which pathogens are active
RESEARCH WARNING, ignored for decades: treating one pathogen in a polymicrobial illness is a recipe for failure. This is why ILADS physicians screen comprehensively; this explains why IDSA guidelines that focus only on Borrelia produce so many "treatment failures."
THE BOTTOM LINE: When you're infected with a dirty needle, treating one poison doesn't cure the rest. The establishment's refusal to acknowledge co-infections isn't just bad science; it's malpractice by design.
The Chronic Lyme War: Why Your Suffering Is Profitable
The controversy over "chronic Lyme" isn't a scientific debate. It's a business decision dressed up as medicine.
IDSA vs ILADS: The Battle Lines
Infectious Diseases Society of America (IDSA):
- Short-course antibiotics (10–28 days maximum)
- Persistent symptoms = "Post-Treatment Lyme Disease Syndrome" (PTLDS)
- View: Antibiotics always work; remaining symptoms are "post-infectious" damage or psychiatric
International Lyme and Associated Diseases Society (ILADS):
- Individualized, longer or repeated courses when infection is suspected
- Recognition that Borrelia can persist despite treatment
- View: Persistent infection is real and treatable
The medical establishment has aggressively sided with IDSA. Why?
Follow The Money: Why Denial Pays
- Long-term treatment = expensive. Insurance companies save billions by limiting treatment to 2–4 weeks
- Liability avoidance. Admitting chronic infection exists opens the door to millions of misdiagnosis lawsuits
- Guideline-driven medicine creates protected revenue streams for guideline authors
PTLDS as a semantics game: By renaming persistent infection as "syndrome" (PTLDS), the establishment:
- Avoids acknowledging treatment failure
- Shifts blame to the patient's body ("post-infectious")
- Justifies denying further antibiotic coverage
- Protects the guideline authors from accountability
THE UNCOMFORTABLE TRUTH: The same playbook used to deny chronic Lyme: dismissing patients as psychiatric, restricting treatment, and attacking dissenting physicians was later perfected on COVID vaccine injury patients. The Lyme community was the testing ground.
For people living with Lyme: calm the fire first (food → inflammation)
A deeper dive into the biochemical triggers of inflammation, and the foods that silently feed the fire, informed by Wahls-style protocols and gut–immune research. Whether you're dealing with autoimmunity, neuroinflammation, chronic fatigue, IBD, MS, arthritis, or post-viral syndromes, removing inflammatory inputs is a power move.
🚫 1) Gluten-containing grains
Gluten → zonulin → leaky gut; LPS translocation; molecular mimicry.
🥛 2) Dairy (esp. conventional A1 dairy)
A1 casein → BCM-7 (gut/brain inflammation); lactase deficits; casein antibodies.
Later (if tolerated): A2 or fermented goat/sheep, exclude in elimination.
🌱 3) Legumes
Lectins bind epithelium; phytates steal minerals; soy adds glyphosate/phytoestrogens; peanuts carry aflatoxins.
Pressure-cooking helps, doesn't erase all anti-nutrients, avoid early.
🍅 4) Nightshades (if sensitive)
Alkaloids (solanine, capsaicin) can irritate gut, activate mast cells, and trigger neurogenic inflammation.
🍬 5) Processed sugars & refined carbs
Glucose spikes → insulin surges → NF-κB/IL-6; dysbiosis; AGEs harm mitochondria, collagen, neurons.
🌽 6) Industrial seed oils
High linoleic acid (ω-6) → pro-inflammatory eicosanoids; easy oxidation → lipid peroxides.
Swap: extra virgin olive oil, coconut oil, ghee, avocado oil, animal fats.
🧈 7) Trans fats
Wreck membranes, insulin signaling, mitochondria.
🚫 Zero is the target.
🧪 8) Artificial additives & preservatives
Mast-cell activation, histamine load; excitotoxins (MSG/aspartame) can worsen neuroinflammation; preservatives distort microbiota.
🍏 9) FODMAPs (for sensitive guts)
Fermentable carbs can fuel IBS/SIBO; raise permeability and mast-cell activity.
Low-FODMAP is a tool, not a lifestyle, use briefly to calm the gut.
Simple swaps you can live with
| Swap this | For this |
|---|---|
| Wheat bread/pastries | Buckwheat, cassava, gluten-free sourdough |
| A1 cow dairy | A2/fermented goat or sheep (after elimination) |
| Seed oils (soy/corn/canola) | Extra virgin olive oil, ghee, avocado oil |
| Refined sugar/HFCS | Berries, 85% dark chocolate, raw honey (sparingly) |
| Nightshades (if sensitive) | Squash, beets, carrots, cucumber |
Polyphenol targets (food first)
| Food | Key compound | Why it's here |
|---|---|---|
| Green tea | EGCG | Angiogenesis + NF-κB modulation |
| Red grapes/blueberries | Resveratrol | EMT/STAT3 control, apoptosis |
| Onions/capers | Quercetin | CSC inhibition, PI3K/Akt |
| Parsley/celery/chamomile | Apigenin | mTOR↓, pro-autophagy |
| Broccoli sprouts | Sulforaphane | Phase II detox (GST), redox support |
30–60 day reset (save this)
- Eliminate: gluten, A1 dairy, legumes, seed oils, sugar, additives (trial nightshades/FODMAPs if symptomatic).
- Add: crucifers/sprouts, green tea, berries, EVOO, spices (turmeric).
- Track daily: sleep, pain (0–10), neuro sx, GI/stools, energy, HR/palps, foods.
- Reintroduce: one item every 3–4 days; note changes at 24/48/72 h.
Genome defense: antimutagens that matter
High-heat meat makes heterocyclic aromatic amines (HAAs), genotoxic. Your counter-punch: crucifers (sulforaphane → GST), curcumin, resveratrol, chlorophyllin/green-tea polyphenols, and fiber to bind/excrete mutagens. That combo down-modulates CYP450 activation, shifts Phase II detox, controls ROS, and tunes gene expression.
- Review of 160+ studies on antimutagenic strategies: https://doi.org/10.1080/10408440091159176
Erich Traub, LCMV & the biowarfare shadow
You want the uncomfortable part? Here it is.
- Erich Traub worked on stealth biological agents designed to evade detection and cause chronic disease.
- LCMV is neurotropic and often misdiagnosed, a template for immune-evasive persistence.
- Lyme as a weaponized platform: allegations of animal passages to refine organisms and keep plausible deniability, "just nature."
- Ticks are perfect vectors: long feed times, painless attachment, direct bloodstream access, broad host range.
- The line between "research" and deployment is thin, and smudged.
Selected papers & reviews (quick links)
Spirochetes in neurodegeneration / brain tissue
- Miklossy J. Alzheimer's disease, a neurospirochetosis. J Neuroinflammation (2011). https://doi.org/10.1186/1742-2094-8-90
- Riviere GR, et al. Oral Treponema in human brain associated with AD. J Alzheimers Dis (2002). https://doi.org/10.3233/jad-2002-4203
- MacDonald AB. Plaques of AD originate from cystic spirochetes. Med Hypotheses (2006). https://doi.org/10.1016/j.mehy.2006.02.035
Persistence / models
- Embers ME, et al. Borrelia persistence post-antibiotics in macaques. PLoS ONE (2012). https://doi.org/10.1371/journal.pone.0029914
- Sapi E, et al. Biofilm phenotype of Borrelia burgdorferi. Eur J Microbiol Immunol (2012). https://doi.org/10.1556/EuJMI.2.2012.4.4
Endothelial mechanics / transmigration
- Niddam AF, et al. Plasma fibronectin stabilizes Borrelia–endothelium catch-bonds under shear. PNAS (2017). https://doi.org/10.1073/pnas.1615007114
Cardiac involvement
- Yeung C, Baranchuk A. Diagnosis and Treatment of Lyme Carditis. J Am Coll Cardiol (2019). https://doi.org/10.1016/j.jacc.2018.11.035
Diagnostics
- Branda JA, et al. Two-tiered testing with C6 ELISA + immunoblot. Clin Infect Dis (2010). https://doi.org/10.1086/648674
- Fallon BA, et al. Repeated IV antibiotics for Lyme encephalopathy, RCT. Neurology (2008). https://doi.org/10.1212/01.WNL.0000284604.61160.2d
Food → barrier & inflammation
- Fasano A. Zonulin and intestinal barrier. Physiol Rev (2011). https://doi.org/10.1152/physrev.00003.2008
- A1 dairy → BCM-7
- Kamiński S, et al. β-casein polymorphism & health. J Appl Genet (2007). https://doi.org/10.1007/BF03195213
- Jinsmaa Y, Yoshikawa M. Enzymatic release of BCM-7. FEBS Lett (1999). https://doi.org/10.1016/S0014-5793(99)01166-4
Lectins / antinutrients
- Pusztai A, Bardocz S. Plant Lectins. Taylor & Francis (1996). https://doi.org/10.1201/9781482295202
- Liener IE. Antinutritional soybean components. Crit Rev Food Sci Nutr (1994). https://doi.org/10.1080/10408399409527653
Aflatoxins
- IARC Monographs, Aflatoxins. https://publications.iarc.fr/
Seed oils / linoleic acid
- Ramsden CE, et al. Dietary LA and CHD outcomes. BMJ (2013). https://doi.org/10.1136/bmj.e8707
- Kaur N, et al. Linoleic acid & inflammation. BBA (2014). https://doi.org/10.1016/j.bbalip.2014.04.001
Sugar → NF-κB / AGEs
- Brownlee M. The pathobiology of AGEs. Physiol Rev (2001). https://doi.org/10.1152/physrev.2001.81.1.1
- Devaraj S, et al. Glucose induces NF-κB activation. AJCN (2002). https://doi.org/10.1093/ajcn/75.1.2
Low-FODMAP (IBS tool)
- Halmos EP, et al. Low-FODMAP reduces IBS symptoms. Gastroenterology (2014). https://doi.org/10.1053/j.gastro.2013.09.046
Antimutagenic nutrition
- HAA antimutagen review (160+ studies). https://doi.org/10.1080/10408440091159176
- Polyphenols vs pancreatic cancer (pathways & CSCs). https://doi.org/10.3390/antiox9080651
- Diet & colorectal cancer (microbiome, epigenetics). https://doi.org/10.3390/nu13010143
- Annual Review of Nutrition (2008), Nutrition & Mutagenesis. https://doi.org/10.1146/annurev.nutr.28.061807.155449
Bottom line
Borrelia in the brain isn't rare, it's ignored. Strip out what feeds inflammation, feed what protects your genome, and let your body show you what the committees won't.
Educational content, not medical advice. Work with a clinician for diagnosis/treatment.