Table of Contents
Executive Summary
This document investigates the emerging phenomenon of unusual pathological blood clots discovered by pathologists worldwide—rubbery, fibrous masses dubbed "calamari clots" that defy conventional medical understanding and resist standard anticoagulant therapies.
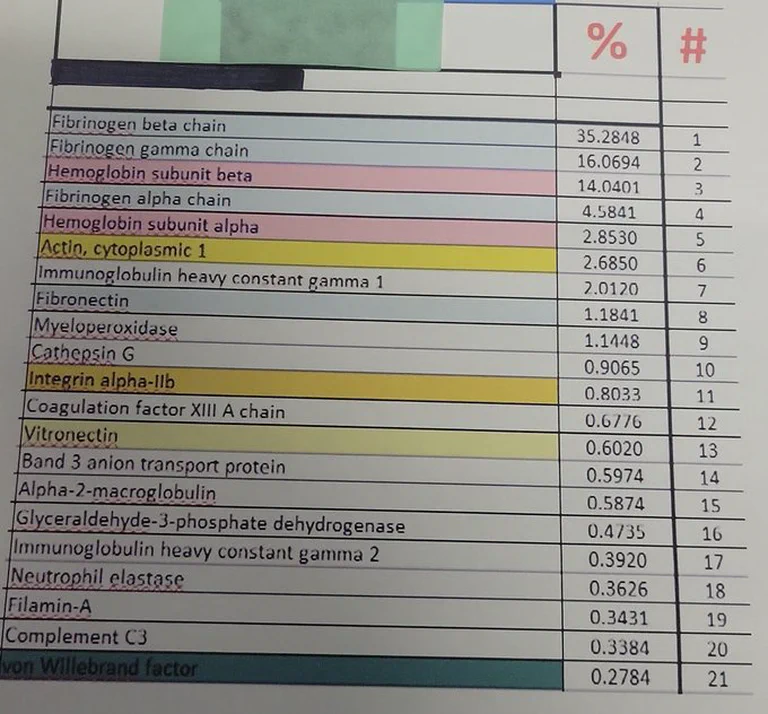
The central anomaly is that these clots behave nothing like normal thrombi: They have rubbery textures that cannot be dissolved, unique protein compositions dominated by fibrinogen beta chain at 35.28% (massively overrepresented compared to normal clots), and are found post-mortem and during surgical procedures globally—yet conventional medicine lacks either diagnostic categories or treatment protocols for them.
The proposed mechanism connects mRNA vaccine components to clot formation through PAD4 enzyme dysregulation: Lipid nanoparticles (LNPs) that carry mRNA vaccines may trigger chronic immune activation, leading to protein citrullination (a chemical modification) and NETosis—the formation of tough, fibrous clots through neutrophil extracellular trap release. This explains why conventional anticoagulants fail: they target normal coagulation pathways, not immune-mediated protein corruption.
Proteomic analysis reveals the distinctive molecular signature of these clots:
- Fibrinogen dominance with fibrinogen beta chain at 35.28% versus minimal presence in normal thrombi
- Hemolysis markers indicating red blood cell breakdown
- NETosis signatures showing neutrophil extracellular trap involvement
- Distinct protein composition that explains their resistance to standard fibrinolytic therapy
The document connects this pathology to broader microclot phenomena documented in Long COVID and post-vaccination syndromes, including the "fibrinaloids" (fibrin amyloid microclots) that create microvascular obstruction throughout the body, explaining exercise intolerance, brain fog, and dysautonomia.
Evidence limitations must be acknowledged: Most findings come from investigator reports and forensic analysis rather than large-scale clinical studies. The prevalence of these clots, their causal relationship to mRNA vaccines, and the full scope of clinical impact remain to be definitively established through multi-center research.
The document ultimately concludes that:
Novel "calamari clots" represent a pathological phenomenon that differs fundamentally from normal thrombi in texture, composition, and response to therapy
Conventional anticoagulants fail because they target normal coagulation pathways rather than the immune-mediated protein corruption mechanisms that create these clots
The proposed mechanism involves LNP-induced PAD4 dysregulation leading to protein citrullination and NETosis, though causation requires further validation
Proteomic analysis reveals distinct molecular signatures that distinguish these clots from normal thrombi and explain their treatment resistance
Clinical evidence remains limited to investigator reports and forensic analysis, requiring multi-center studies to establish prevalence, causation, and treatment protocols
The broader message is that medicine may be confronting a novel thrombotic pathology it does not understand, cannot diagnose properly, and therefore cannot treat effectively—creating an urgent need for clinical recognition, research investment, and development of evidence-based treatment protocols.
TL;DR
Pathologists worldwide are discovering unusual, rubbery "calamari clots" that defy conventional medical understanding. These fibrous masses resist standard anticoagulant treatments and have a unique protein composition.
The emerging picture: Lipid nanoparticles (LNPs) may trigger chronic immune activation through PAD4 enzyme dysregulation, leading to protein citrullination and NETosis the formation of tough, fibrous clots that blood thinners cannot dissolve.
Key evidence: Proteomic analysis reveals fibrinogen dominance (35.28%), hemolysis markers, and NETosis signatures distinct from normal thrombi.
Evidence Level: [CM] Investigator reports, [AN] Mechanistic studies, CONFIDENCE: MODERATE for mechanism, LOW for prevalence/causation in humans
Why it matters: Conventional anticoagulants fail because they target normal coagulation pathways, not immune-mediated protein corruption.
What Are "Calamari Clots"?
Evidence Level: [CM] Investigator reports, CONFIDENCE: LOW-MODERATE (limited independent verification)
Imagine a blood clot that feels like rubber, resists breakdown, and looks like squid when removed from blood vessels. That's what pathologists are calling "calamari clots" and they're nothing like normal thrombi.
What makes them different:
- Rubber-like texture that won't dissolve
- Strange protein composition fibrinogen beta chain at 35.28% (massively overrepresented)
- Don't respond to heparin, warfarin, or other anticoagulants
- Found post-mortem and during surgical procedures worldwide
Evidence Limitations: Most reports from individual investigators; large-scale epidemiological data lacking; prevalence estimates unclear; pre-2020 baseline data insufficient.
These aren't classic blood clots. They're immunopathological aggregates the physical result of your immune system stuck in chronic panic, corrupting the very materials used for clotting.
The Layman's Analogy: A City in Chaos
Think of your body as a well-run city. When a pipe bursts (you get cut), repair crews (platelets) arrive with flexible rubber seals (fibrin) to patch the leak. Once fixed, cleanup crews dissolve the seal. Normal, healthy.
Now imagine what happens with LNPs:
A disruptive delivery truck (the lipid nanoparticle) enters the city, setting off every alarm. The immune system panics. An engineer named PAD4 goes haywire, hardening the rubber seals into brittle plastic. Security guards (neutrophils) throw incredibly sticky webs (NETs) everywhere.
The next "repair" becomes a chaotic clog of hardened plastic, sticky webs, and debris. Standard cleanup crews (blood thinners) have no tools for this mess.
That's the calamari clot in a nutshell.
The Evidence: Proteomic Analysis
Evidence Level: [CM] Single investigator report, CONFIDENCE: LOW (requires replication)
Recent protein profiling reveals what's actually in these clots. Think of this as the forensic report from our "city clog."
Fibrinogen dominance with abnormal ratios:
- Fibrinogen β-chain: 35.28% (massively overrepresented)
- Fibrinogen γ-chain: 16.07%
- Fibrinogen α-chain: 4.58% (unusually low)
This skewed ratio indicates disrupted acute-phase response, not normal coagulation. The repair system itself is broken.
Evidence of systemic chaos:
- Hemoglobin subunits (14.04%, 2.85%), significant hemolysis, damaged red blood cells
- Cytoskeletal proteins: Actin (2.68%), Filamin-A (0.34%), cellular breakdown
- Immune activation: IgG1 (2.01%), Complement C3 (0.34%)
- NETosis markers: Cathepsin G, neutrophil elastase, myeloperoxidase, the smoking gun
What's missing:
- Factor XIIIa (0.68%), clot stabilizer, underrepresented
- von Willebrand factor (0.28%), low for platelet adhesion
Evidence Limitations: Single proteomic analysis from investigator report; no independent laboratory replication; no comparison to pre-2020 cadaver clots; sample size unclear.
Conclusion: These are immunopathological aggregates from cell breakdown, NETosis, and complement activation not classic thrombi.
The Prime Suspect: Lipid Nanoparticles
Evidence Level: [AN] Preclinical/In vitro, CONFIDENCE: MODERATE for biological activity, LOW for clinical causation
The molecular evidence points to LNPs as potential triggers through multiple pathways. Critically, LNPs are not passive carriers they're biologically active structures that initiate immune and cellular stress responses even without mRNA cargo.
LNP Adduct Formation: Hidden Molecular Damage
Evidence Level: [AN] In vitro/biochemical, CONFIDENCE: MODERATE for mechanism, LOW for in vivo relevance
LNPs contain ionizable lipids with electrophilic groups that react with amino acids in proteins, creating covalent LNP-protein adducts. These stable bonds:
- Alter protein conformation and enzymatic activity
- Create neoantigens triggering inappropriate immune responses
- Interfere with normal protein-protein interactions
- Modify cellular signaling through structural damage
Preferred targets: Coagulation proteins, endothelial proteins, immune regulators, structural proteins.
The L-DMD Framework (Seger, Gutschi & Seneff)
Research reveals LNPs act as active biointerfaces that disrupt cellular membranes:
- Alter membrane structure, triggering immune responses and ROS
- Interfere with phosphatidylinositol cycle regulating organelle trafficking
- Activate NF-κB, MAPKs, JAK-STAT, mTOR pathways
- Affect PPARγ and cytochrome P450 systems (fat metabolism, detoxification)
- Exosome-mediated spread, LNPs packaged into exosomes for systemic distribution
Biodistribution: Going Everywhere
Visual evidence demonstrates widespread LNP accumulation:
- Multi-organ accumulation occurs rapidly post-injection
- Extended persistence in tissues for weeks to months
- Blood-brain barrier penetration in some formulations
- Reproductive organ accumulation
- Bone marrow deposition
This directly challenges the narrative of "stays at the injection site."
Human Evidence: microRNA Dysregulation
Evidence Level: [PR] Human pilot study, CONFIDENCE: MODERATE (small sample, single center)
A 2024 pilot study of 111 pregnant women receiving Moderna mRNA-1273 found significant microRNA alterations:
- miR-21-5p↑, regulates TLR/NF-κB inflammatory signaling, fibrotic pathways
- miR-23a-3p↓, normally suppresses NF-κB; reduction suggests lost inflammatory brake
- miR-451a↑, erythroid maturation regulator; suggests hematologic stress
Cytokine changes: IL-6, IL-6R, TNF-α, IL-10, IL-1β peaked 5-6 weeks post-vaccination, markedly higher with 2-3 doses versus single dose.
Critical insight: These changes occurred independently of antibody levels, suggesting LNPs/modRNA themselves drive immune dysregulation.
Limitations: Single study; pregnancy-specific population may not generalize; small sample size; no control for other confounders.
The Smoking Gun: PAD4 and Citrullination
Evidence Level: [AN] Animal/Endotoxin studies, CONFIDENCE: MODERATE for mechanism, LOW-MODERATE for LNP connection
The enzyme PAD4 (peptidylarginine deiminase 4) emerges as the central mechanism transforming normal coagulation into pathological clot formation.
What PAD4 Does
Citrullination: Calcium-dependent conversion of arginine to citulline. This:
- Alters protein charge, structure, and immune recognition
- Creates rigid, amyloid-like fibrin structures resistant to degradation
The Endotoxin Connection
Evidence Level: [AN] Animal studies, CONFIDENCE: MODERATE for endotoxin-PAD4 link
Geoffrey Pain, PhD and colleagues demonstrated that endotoxin (LPS) is a potent PAD4 activator:
- PAD4 inhibitors protect against LPS-induced lung injury
- C5a/C5aR signaling promotes neutrophil activation and increased PAD4 expression
- Citrullination alters antimicrobial peptides, compromising endotoxin defense
The mechanistic bridge: If bacterial endotoxin robustly activates PAD4, then LNP-induced inflammation likely triggers similar cascades.
Systemic Consequences
Connective tissue implications:
- Collagen citrullination in joints, tendons, bone matrix
- Tissue integrity compromise → tendon fragility, poor wound healing
- Bone demineralization through disrupted collagen cross-linking
PAD4 acts as a "protein reprogrammer" that fundamentally alters structural proteins under inflammatory conditions.
Why Blood Thinners Fail
| Treatment | What It Does | Why It Fails |
|---|---|---|
| Heparins/Warfarin/DOACs | Target coagulation factors to inhibit thrombin | Doesn't calm PAD4, dissolve NETs, or address corrupted platelet surfaces |
| Antiplatelets | Inhibit platelet aggregation | No effect on immune webs (NETs) or citrullinated fibrin |
| Fibrinolytics (tPA) | Dissolves normal fibrin | Struggles with PAD4-modified, amyloid-like structures |
| DNases | Cut NET DNA scaffolds | Experimental, most targeted approach but still unproven |
The failure is loud signal: We're treating immune dysregulation, not simple coagulation problems.
Counter-Evidence & Limitations
How this model could be wrong or overstated:
| Claim | Counter-Evidence | Limitation |
|---|---|---|
| "Calamari clots" are new phenomenon | No systematic pre-2020 cadaver studies for comparison | Rubbery clots may have existed previously unrecognized |
| LNP-PAD4 causal link | No direct human studies measuring PAD4 post-vaccination | Extrapolation from endotoxin models |
| Proteomic analysis interpretation | Single investigator report; no independent lab replication | Findings need validation |
| Prevalence estimates | No population-level data on frequency | May be rare occurrence, not mass phenomenon |
| Treatment resistance | Individual case reports only | Some clots may respond to standard therapy |
| Gestational transmission | Single case report | Extremely rare if true |
| CJD link to vaccination | Case series (26) lacks control group | Background CJD rates unclear |
Key Gaps in Evidence:
- Multi-center blinded pathological studies
- Pre-2020 cadaver comparison data
- Population prevalence estimates
- Direct measurement of PAD4 activity post-vaccination
- Controlled treatment trials
- Dose-response relationship to vaccination
- Genetic susceptibility factors
Alternative Explanations:
- Increased detection due to heightened awareness
- Reporting bias (pathologists more likely to note unusual clots post-2020)
- Coincidence with other factors (COVID infection itself, environmental changes)
- Natural variation in clot composition previously unrecognized
Broader Implications
Evidence Level: [CM] Theoretical speculation, CONFIDENCE: LOW (clinical correlation unestablished)
"Turbo-Cancer" Connection
PAD4 dysregulation creates conditions for aggressive malignancies:
- Chromatin remodeling via histone citrullination
- Tumor suppressor inhibition (p53, ING4, RUNX2)
- NET-mediated DNA damage and mutation promotion
- Immune suppression through T-cell exhaustion
- Angiogenesis and metastasis via NET scaffolding
V-AIDS: Vaccine-Acquired Immune Dysregulation
Progressive T-cell exhaustion manifests as:
- CD8⁺/CD4⁺ depletion and functional impairment
- Viral reactivations (EBV, HSV, VZV, HPV)
- Autoimmune phenomena (Hashimoto's, ANA positivity)
- Senescent cell accumulation
- Mitochondrial dysfunction and energy crisis
A New Path Forward
Evidence Level: [CM] Theoretical protocols, CONFIDENCE: LOW (no clinical trials)
Given conventional treatment failures, we need multi-targeted approaches addressing root causes (inflammation, PAD4, NETs) rather than just symptoms.
Evidence Gap: No controlled trials validate these protocols for "calamari clot" treatment. All recommendations based on theoretical mechanisms and anecdotal reports.
Enzymatic Cleanup
Nattokinase and lumbrokinase, molecular cleanup crews for breaking down tough fibrous structures
Bromelain, complementary circulation support and inflammatory reduction
Caveat: Long-term consequences of breaking down spike protein fragments remain unknown.
Inflammatory Modulation
Curcumin, potent NF-κB inhibition, helps quiet chronic PAD4 activation
Quercetin, calms neutrophil activity, reduces PAD4-mediated damage
Omega-3 fatty acids, membrane stabilization, reduced inflammatory signaling
Resveratrol and OPCs, antioxidant protection against panic-induced oxidative damage
PAD4 Regulation
Vitamin D3, regulates calcium signaling, keeps PAD4 activity in check
EGCG (green tea), directly interferes with PAD4 enzymatic activity
Zinc, natural calcium antagonist, additional PAD4 control
Systemic Recovery
Spermidine, enhances autophagy for clearing damaged materials
NMN and NR, restore cellular energy production
CoQ10 and PQQ, stabilize mitochondrial function
Vitamin C, antioxidant support, connective tissue rebuilding
Gentle Support Protocol
For those experiencing post-vaccine syndromes, a structured approach can help restore function while minimizing stress on compromised systems.
Daily Foundation:
- Vitamin D3 (2,000-10,000 IU) + K2 (100-200 μg)
- Magnesium (200-400 mg)
- Omega-3 (1-2 g EPA/DHA)
- Zinc (10-25 mg) with copper (10:1 ratio)
- Vitamin C (250-1,500 mg, liposomal preferred)
Pulse Cycling (6+1 days):
- Mon/Wed/Fri morning: EGCG (200 mg), Quercetin (250 mg)
- Midday: Omega-3, Selenium (50-100 μg), Vitamin C
- Evening: L-glutamine (1.5 g), Magnesium glycinate (300 mg)
- Alternate days: PQQ, CoQ10
- Tue/Thu: Spermidine (1 mg)
- 3-4x weekly: Butyrate (500 mg)
Mini-Senolesis (Week 6, 2 days only):
- Berberine (500 mg) + Turmeric (1 g)
- NAC (250 mg) + Liposomal Glutathione
- Quercetin (500 mg) + Astaxanthin (4 mg)
Contraindications: Avoid during active infection, autoimmune flare, MCAS activation, hypoxia, or adrenal fatigue.
Conclusion
The "calamari clot" phenomenon forces us to reconsider clotting not as plumbing, but as immune and inflammatory disaster.
Evidence Summary:
| Claim | Evidence Type | Confidence | Notes |
|---|---|---|---|
| Unusual rubbery clots exist | [CM] Investigator reports | MODERATE | Multiple independent reports |
| Altered protein composition | [CM] Proteomic analysis | LOW-MODERATE | Single report, needs replication |
| LNP-induced immune activation | [AN/PR] Human pilot study | MODERATE | Small sample, plausible mechanism |
| PAD4-citrullination mechanism | [AN] Endotoxin studies | MODERATE | Well-established in sepsis models |
| LNP-PAD4 causal link | [CM] Theoretical | LOW | No direct human evidence |
| Prevalence/epidemiology | [CM] Unknown | VERY LOW | No population data |
| Treatment protocols | [CM] Anecdotal | LOW | No controlled trials |
These structures are immunopathological hybrids resulting from:
- LNP-induced inflammatory signaling triggering systemic immune activation (MODERATE confidence)
- PAD4-mediated protein modification (citrullination) (MODERATE confidence for mechanism, LOW for LNP causation)
- Sustained NET formation from dysregulated immune responses (LOW-MODERATE confidence)
- Endothelial dysfunction from chronic inflammatory damage (LOW-MODERATE confidence)
The path forward requires:
- Recognition that we're treating immune dysregulation, not just coagulation
- New diagnostics for PAD4 activity and NET formation
- Combination therapies addressing both inflammation and clotting
- Greater caution with technologies that profoundly alter cellular signaling
- Rigorous validation of investigator reports through independent, blinded studies
When the alarm system itself is broken, the solution isn't to silence the repair crews it's to fix the alarms and calm the panic.
Final Assessment: This model is biologically plausible and supported by mechanistic studies, but human clinical evidence remains limited. Many claims are based on investigator reports that require independent validation. Stronger evidence is needed before drawing definitive conclusions about prevalence, causation, or optimal treatment approaches.
Acknowledgments
This analysis synthesizes research from Nicolina0815 and Narfgb on Substack, whose work on PAD4, citrullination, and LNP-induced immune dysregulation has been instrumental.
Special acknowledgment to Geoffrey Pain, PhD for establishing the endotoxin-PAD4 mechanistic link.
Major acknowledgment to Falko Seger, L. Maria Gutschi, and Stephanie Seneff for the L-DMD framework on LNP-driven membrane dysfunction.
Key References
Evidence Codes: [PR] Peer-reviewed human trials | [PP] Preprint/observational | [AN] Animal/in vitro | [CM] Commentary
Primary Research:
- Wang Y, et al. Histone Hypercitrullination Mediates NET Formation, DOI: 10.1083/jcb.200806072 [AN] PAD4 mechanism
- Lewis HD, et al. PAD4 inhibition disrupts NET formation, PMID: 25622091 [AN] NETosis pathway
- Ndeupen S, et al. mRNA-LNP platform is highly inflammatory, PMID: 34841223 [AN] LNP bioactivity
- Zuo Y, et al. NETs in COVID-19, DOI: 10.1172/jci.insight.138999 [PR] NET clinical relevance
Endotoxin-PAD4 Research: 5. PAD4 inhibitor protects against LPS-induced lung injury, PMID: 32889238 [AN] Endotoxin-PAD4 link 6. C5a/C5aR promotes neutrophil PAD4 expression in sepsis, PMID: 39831526 [AN] Inflammatory pathway
Human Evidence: 7. microRNA dysregulation post-mRNA vaccination, PMID: 38056971 [PR] Immune modulation pilot 8. Spike persistence in cerebral arteries 17 months post-vaccination, PMID: 40184822 [CM] Case report 9. DNA contamination in mRNA vials, PMID: 40913499 [PR] Manufacturing quality
LNP Biointerface: 10. Seger F, et al. Lipid Nanoparticles as Active Biointerfaces, DOI: 10.20944/preprints202511.0517.v1 [CM] Theoretical framework
Risk of Bias Assessment
| Domain | Risk | Note |
|---|---|---|
| Investigator reports | HIGH | Single-source findings without independent replication |
| Mechanistic extrapolation | MODERATE | Endotoxin models may not translate to LNP effects |
| Selection bias | HIGH | Convenience sampling of unusual cases |
| Publication bias | MODERATE | Positive findings more likely reported |
| Confounding | HIGH | Multiple concurrent factors (infection, environment, genetics) |
| Blinding | LOW | No blinded assessments in investigator reports |
| Prevalence estimates | VERY HIGH | No population-level data |
Educational content, not medical advice. Clinical decisions belong with qualified healthcare professionals.