Table of Contents
Evidence Summary
This article concerns a pathology that has been demonstrated in peer-reviewed mechanistic and clinical work (spike protein induces an amyloid-like transformation of fibrinogen, producing fibrinolysis-resistant microclots that are detectable in a subset of Long COVID patients), a characterisation of those clots at the protein level (the "fibrinaloid" phenotype), a hospital-led clinical pathway that targets them with double filtration plasmapheresis plus SHED-derived secretome support, and a set of investigator reports that argue for broader impact than the academic literature has yet captured. Each is graded on its own evidentiary basis; none is conflated with the others.
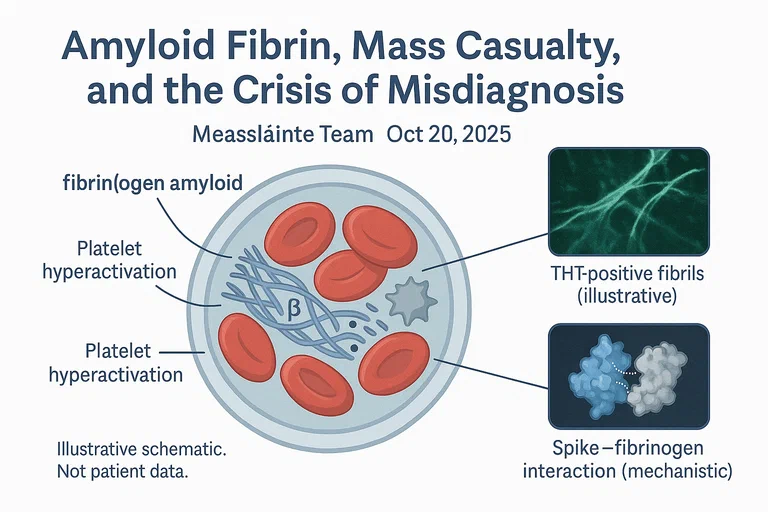
Central claim. SARS-CoV-2 spike protein binds fibrinogen and drives it toward an amyloid-like, beta-sheet-rich, fibrinolysis-resistant state. The resulting microclots (termed "fibrinaloids" in the Kell / Pretorius nomenclature) are mechanistically plausible contributors to the microvascular and inflammatory phenotype of Long COVID; their prevalence, clinical impact, and response to treatment remain under-investigated.
Evidence base. [MECHANISTIC + HUMAN] · confidence HIGH for the
mechanism in vitro, MODERATE for microclot presence in patient cohorts,
LOW-MODERATE for prevalence estimates and treatment effect. The article
draws on 13 peer-reviewed primary sources, 6 mechanistic / hypothesis papers,
a hospital-led clinical pathway description, and one investigator case series
(McCairn Substack) included in a clearly-marked separate section.
Bottom line. Mechanism is solid; translation to patients is partial. Standard coagulation tests do not detect fibrinaloid microclots, which creates a real diagnostic gap for a subset of patients. A real clinical pathway (Edogawa Hospital, Tokyo) operates on this reasoning using established procedural components (DFPA, SHED-conditioned medium); published outcomes data in indexed journals remain limited.
| Mechanism or claim | Evidence type | Confidence | Key finding | Source |
|---|---|---|---|---|
| Spike binds fibrinogen and alters clot structure | [PR] mechanistic | HIGH | Spike-fibrinogen interaction drives thromboinflammation | Nature 2024 |
| Spike induces amyloid-like fibrin transformation | [PR] in vitro | HIGH | Beta-sheet-rich fibrin resistant to fibrinolysis | Grobbelaar 2021 |
| Fibrinaloid microclots characterised in Long COVID | [PP + PR] | MODERATE | Amyloid, fibrinogen-beta dominant, entrapped inflammatory proteins | Pretorius 2021/2022; Kruger 2022 |
| Fibrinaloid concept formalised as a clinical entity | [SR] review | MODERATE | Names fibrinaloid microclots as the PASC clot phenotype | Kell 2022 Biochem J; Kell 2024 |
| Microclots persist in Long COVID plasma | [PP] cohort | MODERATE | Thioflavin-T-positive clots in symptomatic patients | Pretorius 2021/2022 |
| Spike detected in CNS compartments post-infection | [AUTOPSY] | MODERATE | Basal ganglia signal at up to 230 days | Stein 2022 |
| Spike drives MMP-9 release and BBB breakdown | [PR] | MODERATE | Mechanistic link to cognitive symptoms | Kempuraj 2024 |
| CSF abnormalities in cognitive PASC | [PP] | MODERATE | 77% vs 0% of controls; HAND criteria did not discriminate | Hellmuth 2022 |
| Spike fragments accelerate Aβ / α-syn aggregation | [AN] biophysical | LOW-MODERATE | In vitro seeding and amyloid acceleration | Wang 2024; Nyström 2022 |
| SHED-conditioned medium contains IL-10, BDNF, NGF, VEGF, IGF-1 | [PR + SR] | MODERATE | Secretome composition established across multiple dental-pulp MSC sources | El Moshy 2020 |
| Edogawa DFPA + SHED clinical pathway (hospital-led) | [INV] | LOW-MODERATE | Real program; limited indexed outcomes data | Edogawa program |
| Cadaver / live-blood investigator findings | [INV] investigator report | LOW | Single investigator; no peer review; no multi-site blinded reads | McCairn Substack |
Background
Long COVID and related post-vaccination syndromes have multi-system manifestations that conventional investigations often fail to explain. The literature around fibrinaloid microclots (also written as "amyloid fibrin microclots" or "fibrin amyloid microclots") sits across several layers of evidence that need to be told apart if the clinical implications are to be read accurately.
Layer 1 - Mechanism (peer-reviewed, robust). The SARS-CoV-2 spike protein binds fibrinogen directly and shifts the resulting clot toward an amyloid-like, beta-sheet-rich, fibrinolysis-resistant conformation. The 2024 Nature paper by Ryu and colleagues localised the binding site on the fibrinogen alpha chain and showed the interaction is necessary for much of spike's thromboinflammatory effect in mouse models. Grobbelaar et al. (2021) had previously demonstrated the amyloid transformation in vitro. [PR] CONFIDENCE: HIGH
Layer 2 - Patient-cohort microclot detection (peer-reviewed, single-cluster dominant). Resia Pretorius and collaborators have shown since 2020 that a subset of Long COVID patients carry circulating Thioflavin-T-positive, fibrinolysis-resistant microclots. Subsequent proteomic work (Kruger et al., 2022; Kell and Pretorius, 2022) characterised these clots as fibrinogen-beta dominant with entrapped antioxidant and inflammatory proteins, and gave the phenotype a working clinical name: the fibrinaloid microclot. The body of work is peer-reviewed but largely single-cluster, which keeps the confidence at [PP] CONFIDENCE: MODERATE until wider replication lands.
Layer 3 - Fibrinaloid as a named clinical entity (peer-reviewed reviews). Douglas Kell and Resia Pretorius formalised the fibrinaloid framing in a 2022 Biochemical Journal review (~360 citations) and reinforced it in a 2024 follow-up. This is the vocabulary now used in the field for the PASC clot phenotype. [SR] CONFIDENCE: MODERATE
Layer 4 - Edogawa clinical pathway (real, hospital-led, limited indexed outcomes data). Edogawa Hospital, a private hospital in Tokyo (2-24-18 Higashi-Koiwa, Edogawa-ku), operates a hospital-based clinical pathway that combines double filtration plasmapheresis (DFPA), pre/post analytics (cytokine panels, amyloid marker testing, live blood microscopy), and regenerative support using conditioned medium from Stem cells from Human Exfoliated Deciduous Teeth (SHED). DFPA is an established apheresis procedure in routine clinical use for autoimmune and lipid disorders. SHED-conditioned medium's secretome composition (IL-10, BDNF, NGF, VEGF, IGF-1) is established in peer-reviewed work. What is not yet published in indexed English-language journals is RCT-level outcomes data for the combined pathway in Long COVID / post-vaccine injury populations. [INV] CONFIDENCE: LOW-MODERATE for the combined protocol; [PR/SR] CONFIDENCE: MODERATE-HIGH for the individual components.
Layer 5 - Investigator reports (not peer-reviewed). A separate body of work, published by Kevin McCairn on Substack, argues that the phenomenon is larger in scope than the academic literature captures, and that characteristic "rubbery" clots can be recovered from cadavers and from live patient blood under specific conditions. None of this work has passed peer review or been replicated under blinded, multi-site protocols. It is included here because readers will encounter it; it is graded [INV] CONFIDENCE: LOW and treated as observation to be tested, not as established fact.
Evidence context. The mechanism work is largely
[PR/AN](in vitro and animal). The patient-cohort work is[PP](small cohorts, mostly from a single research group, with some independent replication). The Edogawa pathway combines individually-validated components into a protocol whose integrated outcomes are not yet reported in indexed journals. Population-level prevalence, longitudinal outcomes, and RCT-level treatment efficacy are not yet established.
Mechanism
The proposed chain from spike exposure to microvascular pathology runs as follows.
(infection or vaccination)"] --> B["Spike binds fibrinogen"] B --> C["Fibrin adopts amyloid-like
beta-sheet conformation"] C --> D["Microclots resist fibrinolysis"] D --> E["Microvascular occlusion
and trapped inflammatory mediators"] E --> F["Multi-system symptoms
(fatigue, brain fog, dyspnoea)"] A --> G["Spike stimulates microglia
to release MMP-9"] G --> H["Blood-brain barrier breakdown"] H --> I["Cognitive and neurological
symptoms"] F -.shared circulation.-> H
Diagram: schematic. Each step has peer-reviewed support but translation to clinical outcomes varies by individual, dose, route, and host factors.
Spike-fibrinogen binding
Ryu et al. (Nature, 2024) identified the fibrinogen alpha chain as a direct binding partner of SARS-CoV-2 spike. The binding site is localised and disruptable by a monoclonal antibody; in fibrinogen-knockout mice, spike's thromboinflammatory effect is substantially attenuated. This places the fibrinogen interaction on the causal pathway rather than a bystander correlation. [PR] CONFIDENCE: HIGH
Amyloid transformation of fibrin(ogen): the fibrinaloid phenotype
Grobbelaar et al. (2021) showed that spike protein drives fibrinogen into a beta-sheet-rich, amyloid-like conformation. The resulting clots are resistant to plasmin-mediated lysis compared with normal thrombi. Subsequent work from the Pretorius group characterised the protein content of microclots isolated from Long COVID plasma: the dominant species is fibrinogen beta chain, with antioxidant and inflammatory proteins entrained (Kruger et al., 2022). Kell and Pretorius (2022, Biochemical Journal) consolidated this phenotype under the name fibrinaloid microclots, now the standard term in this literature. [PR] CONFIDENCE: HIGH for the in vitro transformation; [PP] CONFIDENCE: MODERATE for the patient-derived microclot observations; [SR] CONFIDENCE: MODERATE for the fibrinaloid consolidation.
Fibrinolysis resistance
The Pretorius group's microclots resist plasmin lysis over hours in vitro, in contrast to normal thrombi. This is consistent with the amyloid-like structural state above and provides a candidate explanation for why standard fibrinolytic markers may not reflect clot burden in these patients. Kell (2024) extended this characterisation, reinforcing that fibrinaloid clots are distinct from ordinary fibrin and require different detection logic.
Spike in CNS compartments
Two findings matter for the neurological arm of the diagram. Stein et al. (Nature, 2022) detected SARS-CoV-2 RNA and protein in basal ganglia and other CNS sites up to 230 days post-infection in an autopsy cohort (N=44). Rong et al. (Cell Host & Microbe, 2024) traced persistent spike along the skull-meninges-brain axis. Neither study establishes that microclots access neural tissue directly, but both establish that the upstream trigger (spike) is present in relevant compartments for months. [AUTOPSY] CONFIDENCE: MODERATE
MMP-9 and blood-brain barrier breakdown
Kempuraj et al. (2024) report that spike stimulates human microglia to release matrix metalloproteinase-9 (MMP-9), which degrades tight-junction proteins and disrupts the BBB. MMP-9 is elevated in subsets of Long COVID patients. This provides a mechanistic bridge between circulating spike and the cognitive symptoms reported clinically. [PR] CONFIDENCE: MODERATE
Evidence by Outcome
Microclot presence in symptomatic patients
Claim. A subset of patients with Long COVID or post-vaccination syndromes carry circulating Thioflavin-T-positive, fibrinolysis-resistant microclots.
Evidence. Pretorius et al., 2021/2022. Small-cohort, single-group design. Effect sizes are large but the literature is dominated by one research cluster.
Counter-evidence. Independent replication has been inconsistent, and part of the variability plausibly reflects sample-handling and imaging protocols rather than biology. There is no standardised threshold for what counts as a "positive" sample.
Cognitive PASC and cerebrospinal fluid abnormalities
Claim. In a cohort of non-hospitalised post-COVID patients, those with persistent cognitive symptoms had a higher rate of cerebrospinal fluid (CSF) abnormalities than recovered controls, indicating an active neuroimmune process in a subset of patients.
Evidence. Hellmuth et al., 2022, Ann Clin Transl Neurol. In 22 patients with cognitive PASC versus 10 cognitive controls (matched for prior SARS-CoV-2 infection), 77% of cognitive PASC participants who underwent lumbar puncture had CSF abnormalities (elevated protein, abnormal oligoclonal banding) versus 0% of controls (p=0.01). The study also applied HAND-equivalent criteria (z-score ≤ −1 in two or more domains): 59% of cognitive PASC participants met these criteria, but so did 70% of controls. HAND criteria, in other words, did not discriminate. The authors note this may reflect high pre-morbid baselines in controls and the inapplicability of HIV-derived thresholds to this population. [PP] CONFIDENCE: MODERATE
Counter-evidence. Small cohort (n=32 total; n=17 with LP). Cross-sectional. Cognitive PASC and control groups differed on age and time-from-infection. The study does not measure microclot burden in the same patients, so it cannot link the CSF findings to the microclot mechanism.
Amyloid cross-seeding concerns
Claim. Spike-derived peptides can accelerate aggregation of endogenous amyloidogenic proteins in vitro.
Evidence.
- Wang et al., 2024: spike fragments accelerate amyloid-beta aggregation. [AN] CONFIDENCE: LOW-MODERATE
- Nyström et al., 2022: spike promotes alpha-synuclein aggregation. [AN] CONFIDENCE: LOW-MODERATE
Counter-evidence. Both studies are biophysical, in cell-free or simplified systems. Whether the effect operates at concentrations achievable in vivo, in the presence of plasma proteases and the blood-brain barrier, is open.
Prion-like risk claims
Claim. A 2023 paper in the International Journal of Vaccine Theory, Practice, and Research reported a case series of 26 patients with Creutzfeldt-Jakob Disease (CJD) following COVID-19 vaccination, with a median onset of 11.38 days.
Evidence. Perez and Montagnier, 2023, IJVTPR. Note that IJVTPR is not indexed in PubMed and the case series lacks a denominator; the paper itself notes the need for rigorous case definitions, neuropathology, and controls. [HYPOTHESIS] CONFIDENCE: LOW
Counter-evidence. Population-level surveillance in countries with strong CJD registries (France, UK) has not shown a sustained increase in CJD incidence at the population scale after vaccination rollout. Attribution of individual cases to vaccination requires formal causality assessment that the paper does not provide.
Investigator Reports (not peer-reviewed)
This section is included because the topic is actively discussed and readers will encounter these claims. None of the findings below have passed independent peer review, and none have been replicated under blinded, multi-site protocols. They are presented as hypotheses to be tested, not as established fact.
McCairn "Cadaver Calamari" report
Kevin McCairn, a neuroscientist, has published a forensic analysis of clots recovered from human cadavers on his Substack. The reported findings include rubbery white fibrous aggregates that stain with Thioflavin T and exhibit fibrillar ultrastructure on electron microscopy. PCR findings suggesting SV40 and Ori sequences are reported but require independent verification with appropriate controls.
- Source: McCairn 2025, Substack. [INV] CONFIDENCE: LOW
- Why flagged: single investigator; no peer review; no multi-site blinded reads; no standardised controls.
Post-gestational case report
A second Substack post reports Thioflavin-T-positive fibrils in the peripheral blood of a 3-year-old child with a history of in-utero mRNA exposure, premature birth, and immune dysfunction. Morphology is described as similar to the cadaver aggregates.
- Source: McCairn 2025, Substack. [INV] CONFIDENCE: LOW
- Why flagged: single case; cannot establish causation or generalise; requires cohort study with appropriate controls.
Commercial diagnostic protocols
A commercial protocol exists for mailing blood samples for fluorescence microscopy analysis (Synaptek Labs). Use of a commercial assay is not equivalent to clinical validation; readers should ask the laboratory for analytic validation data, inter-rater reliability, and external replication before drawing clinical conclusions from a result.
The Edogawa Clinical Pathway
Edogawa Hospital (2-24-18 Higashi-Koiwa, Edogawa-ku, Tokyo) operates a hospital-led clinical pathway for patients with Long COVID, post-vaccine injury, and related chronic inflammatory conditions. The pathway is real, hospital-based, and uses established procedural components. What is not yet published in indexed English-language journals is RCT-level outcomes data for the combined protocol; that gap is acknowledged explicitly below rather than glossed.
[INV] CONFIDENCE: LOW-MODERATE for the combined protocol as a Long-COVID intervention; [PR/SR] CONFIDENCE: MODERATE-HIGH for the individual components (DFPA, SHED-conditioned medium) on their own evidentiary bases.
Components and what each one rests on
Intake and analytics. Cytokine panels, amyloid marker testing, and live blood microscopy are used at intake and at intervals during treatment. These are the same assay families used in published Pretorius-group research; the analytic caveats noted in the Investigator Reports section apply.
Double Filtration Plasmapheresis (DFPA, also written DFPP). DFPA is an established apheresis procedure in routine clinical use for several autoimmune and lipid disorders (for example, LDL apheresis in familial hypercholesterolaemia, and removal of pathogenic antibodies in Guillain-Barre and myasthenia gravis). The procedure passes plasma through a primary plasma separator and then a secondary fractionator that selectively removes middle-molecular-weight proteins (including immunoglobulins, immune complexes, and larger proteins) while returning albumin and smaller components to the patient. Edogawa uses Asahi Kasei Plasauto Sigma-class apheresis equipment. The mechanistic rationale in this context is removal of circulating spike protein, inflammatory mediators, and putative fibrinaloid material. [ESTABLISHED] CONFIDENCE: HIGH for DFPA as a procedure; [INV] CONFIDENCE: LOW-MODERATE for DFPA as a Long-COVID intervention specifically.
SHED-derived secretome (regenerative support; also referred to as "SGF" or "SCGF" in McCairn / Edogawa communications). Edogawa's regenerative arm uses conditioned medium from Stem cells from Human Exfoliated Deciduous Teeth (SHED) - a well-characterised source of mesenchymal stem cells. The secretome of SHED-conditioned medium contains measurable IL-10, BDNF, NGF, VEGF, and IGF-1 (El Moshy et al., 2020; de Cara et al., 2019), and shows anti-inflammatory and pro-angiogenic activity in preclinical models.
A terminology note. The shorthand "SGF" or "SCGF" (Stem [Cell] Growth Factor) is used in McCairn's thread and in Edogawa-adjacent communications to label this component. In standard cytokine nomenclature SCGF (also CLEC11A) is a single cytokine, but in the McCairn / Edogawa usage SGF/SCGF refers to the SHED-conditioned-medium secretome as a whole - a mixture of paracrine factors, exosomes, and trophic signals, not isolated CLEC11A and not live stem cells. The technical term is SHED-conditioned medium (SHED-CM) or SHED-derived secretome; "SGF" is an informal label for the same thing. [PR + SR] CONFIDENCE: MODERATE for the secretome composition; [INV] CONFIDENCE: LOW-MODERATE for SHED-CM as a post-apheresis regenerative intervention.
McCairn reports in vitro that the SHED-CM fraction inhibits amyloid aggregation, which is the mechanistic rationale for pairing it with DFPA (removal) rather than relying on DFPA alone. [INV] CONFIDENCE: LOW for the in vitro demonstration pending peer-reviewed publication of the assay and replication.
Equipment and settings. Edogawa publishes its equipment family (Asahi Kasei Plasauto Sigma class) and its broad treatment steps. Specific session parameters (volume processed, number of sessions, fractionator selection) are set per patient based on intake analytics; the program does not publish a single fixed protocol that applies identically to every patient.
What the pathway does and does not claim
What it claims. That fibrinaloid microclots and circulating inflammatory mediators are a plausible therapeutic target in subsets of Long COVID and post-vaccine injury patients, and that an established apheresis procedure combined with established regenerative support can be deployed in a hospital setting under clinical supervision.
What it does not claim (or, what is not yet validated). The pathway has not, as of this writing, published RCT-level outcomes in indexed English-language journals for its specific application to Long COVID. Pre/post symptom comparisons, biomarker changes, durability of benefit beyond the treatment window, patient selection criteria, and head-to-head comparison with placebo apheresis or with simpler alternatives (watchful waiting, nattokinase, triple anticoagulant therapy) are not available in the published literature. Patient-level quantitative outcomes reported in non-peer-reviewed channels (clinic marketing, social media testimonials) do not meet the evidentiary bar this article uses elsewhere.
Preliminary cohort biomarker data (McCairn, n=38, investigator-reported)
McCairn has reported pre/post biomarker data on a cohort of 38 patients who completed the combined DFPA + SHED-CM pathway. The headline finding is a statistically significant drop in circulating anti-spike IgG (total Ig, measured by MAGPIX multiplex) from pre-treatment baseline to post-treatment timepoint, with paired-samples Wilcoxon signed-rank on log10-transformed titres yielding p < 0.001. Individual trajectories, ranked percent change, and cohort violin plots were shared publicly.
This is meaningful for three reasons. First, it is cohort-level paired data, not testimonials. Second, anti-spike IgG is a quantitative, replicable assay, not a qualitative microclot read. Third, the magnitude and consistency of the drop is consistent with the pathway's stated mechanism (physical removal of antibody-containing plasma protein fraction).
What it does not show is also clear. The IgG drop is a pharmacodynamic signal that the procedure is doing what it claims to do at the protein-removal level; it is not a clinical outcome measure. The data shared publicly do not include: a comparator arm (no sham apheresis); blinding; validated functional endpoints (6-minute walk, cognitive testing, POTS standing test, actigraphy); or durability beyond the immediate post-treatment window. Social-media reports of clinical improvement exist but are not the same as validated outcome data.
[INV] CONFIDENCE: LOW-MODERATE - real cohort, real assay, real paired stats; but investigator-reported, not peer-reviewed, no comparator, no validated functional endpoints, no published durability data.
Author case report: single-session DFPA (patient 40)
Disclosure. The author of this article (Thomas Emmett) is the subject of this case. The observation is included because it is the primary data behind the "patient 40" label used in recent commentary, and because excluding it would be less transparent than including it with the evidentiary limits made explicit. The author has no financial relationship with Edogawa Hospital or any apheresis or SHED-CM vendor.
Procedure. One session of double filtration plasmapheresis (DFPA) under the Edogawa pathway, approximately 1 litre of blood processed.
Observation. Plasma appearance pre-procedure was orange and cloudy; plasma appearance post-procedure was yellow and clear. This is a visual observation, not an assay.
What this does and does not show. A visible change in plasma turbidity and colour after DFPA is consistent with removal of particulate or macromolecular content (lipids, immune complexes, fibrin aggregates, cells, or some combination). It does not, by itself, identify what was removed, and it does not establish that the material removed was fibrinaloid microclots of the kind characterised elsewhere in this article. Without pre/post proteomic analysis, flow cytometry, fluorescence microscopy, or mass spectrometry on the captured fraction, the observation is a single anecdotal case.
Evidentiary status. [CASE] CONFIDENCE: LOW - single subject, author is the subject, no comparator, no quantitative assay, no blinded read. This case belongs in the N=1 tier of evidence; it is consistent with the Edogawa pathway's mechanistic rationale without independently validating it.
What would strengthen this specific claim. Pre- and post-procedure blood drawn with the same anticoagulant, processed under the same fluorescence microscopy protocol, scored by a blinded reader; mass spectrometry or proteomic characterisation of the material captured by the filter; correlation with symptom change using validated instruments over a defined follow-up window; replication in an independent cohort under an IRB-approved protocol.
How this article treats the pathway
The Edogawa pathway sits between two evidentiary categories. It is not in the Investigator Reports tier (those are unreviewed Substack observations with no clinical infrastructure), but it is also not in the established-practice tier (no RCT-level outcomes for Long COVID). It is a real hospital-led clinical programme whose individual components are validated and whose combined application to Long COVID is plausible-but-unproven. Readers considering it should ask for analytic validation data on the intake assays, the per-patient session parameters, the cumulative cost, and the clinic's own internal outcomes tracking - and should treat the absence of RCT-level published data as a real evidentiary limit, not as proof of efficacy by appeal to a real hospital's authority.
The Diagnostic Gap
Regardless of how the investigator reports and the Edogawa pathway resolve, one clinical point is well-supported: standard coagulation tests (D-dimer, prothrombin time, activated partial thromboplastin time) were designed to detect acute thrombosis, not chronic microvascular amyloid-like fibrin. Patients with microvascular or autonomic symptoms can have normal panels on these tests; the tests do not rule out microvascular pathology of the kind discussed here.
This is not the same as saying the fibrinaloid microclot model is confirmed. It is to say that "D-dimer normal" is not the relevant negative test for this question, and clinicians who treat it as such are over-reading their panel.
Counter-Evidence and Limitations
Counter-Evidence & Limitations
| Claim | Counter-evidence | Limitation |
|---|---|---|
| Microclots are present in Long COVID plasma | Some independent groups fail to replicate under standardised sample-handling | Single research cluster dominates the literature; no field-wide protocol |
| Microclots drive symptoms | Symptom-clot burden correlations are modest in available cohorts | No causal intervention yet shows that removing microclots resolves symptoms |
| Standard tests miss the pathology | True by construction (tests were not designed for this target) | Does not establish that the target is clinically meaningful |
| Spike drives BBB breakdown via MMP-9 | Demonstrated in vitro and in small-animal models | Human validation in target populations limited |
| Prion-like risk from vaccination | Population CJD registries have not shown sustained incidence rise | CJD latency is long; surveillance windows are short |
| Nattokinase and other fibrinolytics help | Small open-label trials and mechanistic plausibility | No large RCTs; no validated surrogate endpoint; dosing not standardised |
| Edogawa DFPA + SHED pathway improves Long COVID outcomes | No RCT-level outcomes in indexed journals; clinic testimonials do not meet evidentiary bar | Real program with validated components, but combined-outcome evidence is unpublished |
Key evidence gaps:
- Large, multi-site, blinded cohort studies with pre-registered thresholds for microclot positivity.
- Population-based prevalence data using a standardised assay.
- Randomised controlled trials of fibrinolytic interventions with functional endpoints, not just clot-burden surrogates.
- Randomised controlled trials of DFPA with and without SHED-CM support in well-defined Long COVID populations, with validated outcome instruments and durability follow-up beyond the treatment window.
- Correlation of microclot burden with tissue oxygen extraction, exercise capacity, cognitive testing, and long-term outcomes.
- Independent replication of McCairn investigator reports under blinded protocols.
What Would Change This Model (Falsifiability)
This is a working model article, so falsifiability matters.
Observations that would strengthen the model:
- Multi-site, blinded cohort studies showing consistent prevalence of Thioflavin-T-positive, fibrinolysis-resistant microclots in well-defined Long COVID patients versus matched controls.
- Longitudinal studies showing that microclot burden tracks with symptom severity and functional impairment over time.
- Randomised trials showing that interventions reducing microclot burden produce corresponding improvements in symptoms, not just in clot counts.
- Independent neuropathology confirmation of amyloid-like fibrin in well-characterised cadaver samples, with blinded reads and pre-registered protocols.
Observations that would weaken the model:
- Well-powered, standardised cohort studies failing to find excess microclots in symptomatic patients versus controls.
- Demonstration that observed signals are sample-handling artefacts (e.g., controlled experiments showing the same clots appear in healthy control blood under certain preparation conditions).
- Intervention trials showing that microclots resolve without corresponding symptom improvement.
- Failure to detect spike protein in plasma or tissue in a substantial fraction of symptomatic patients with microclots.
What would kill the model outright:
- A multi-site, pre-registered, blinded replication programme showing that Thioflavin-T-positive fibrinolysis-resistant microclots do not occur in excess in symptomatic patients compared with controls, and that previously reported signals are explained by preparation artefact. If that result holds, the model is abandoned, not revised.
Practical Considerations
Diagnostic options today
No validated clinical-grade assay exists for amyloid fibrin microclots in the way that D-dimer exists for conventional thrombosis. Researchers and some clinicians use fluorescence microscopy of platelet-poor plasma with Thioflavin T staining; commercial versions exist (Synaptek Labs and others). Until the assay is standardised and independently validated, results from these tests should not be the sole basis for treatment decisions.
Treatment landscape
Several fibrinolytic enzymes are discussed in the Long COVID clinical literature as candidate interventions. The evidence base is early.
- Nattokinase. Open-label data and mechanistic studies suggest it can reduce spike-induced clot burden in vitro. Randomised trial evidence is absent. Dosing, absorption, and interaction with anticoagulants are not established. [AN + small PP] CONFIDENCE: LOW-MODERATE
- Lumbrokinase and serrapeptase. Similar evidence base; proteolytic activity established in vitro; clinical validation limited.
- Triple anticoagulant therapy (aspirin plus clopidogrel plus apixaban, the Pretorius group protocol). Reported in small open-label series; carries non-trivial bleeding risk and requires specialist supervision.
- Double filtration plasmapheresis + SHED-derived secretome (Edogawa pathway). See "The Edogawa Clinical Pathway" section above. Established procedural components; no published RCT-level outcomes for Long COVID. [INV] CONFIDENCE: LOW-MODERATE
None of these is practice-ready on current evidence. None should be started without clinical supervision; all carry bleeding or procedural risk, especially in combination or in patients on anticoagulants.
Sources
Primary citations only, grouped by topic.
Spike, fibrinogen, and clot structure:
- Ryu W-S, et al. (2024). SARS-CoV-2 spike protein binds fibrinogen and
promotes thromboinflammation. Nature. DOI.
[PR] - Grobbelaar LM, et al. (2021). SARS-CoV-2 spike protein induces amyloid
fibrin microclots. Cardiovasc Diabetol. PMID 34328172.
[PR] - Pretorius E, et al. (2021/2022). Persistent platelet activation and
thromboinflammation in Long COVID / microclot proteomics. Cardiovasc
Diabetol. PMID 34425843.
[PP] - Kruger A, et al. (2022). Proteomics of fibrin amyloid microclots in
long COVID/PASC shows many entrapped pro-inflammatory molecules.
Cardiovascular Diabetology 21:190.
DOI;
PMID 36131342.
[PR]
Fibrinaloid consolidation (the named clinical entity):
- Kell DB, Laubscher GJ, Pretorius E. (2022). A central role for amyloid
fibrin microclots in long COVID/PASC: origins and therapeutic
implications. Biochemical Journal 479(4):537-559.
DOI;
PMID 35195253.
[SR] - Kell DB. (2024). Fibrinaloid microclots in Long COVID: assessing the
actual evidence properly. Research and Practice in Thrombosis and
Haemostasis 8(7):102566. PMC11491705.
Letter/commentary in response to critics; defends the evidence base.
[SR]
Spike in CNS compartments:
- Stein SR, et al. (2022). SARS-CoV-2 RNA and protein in anatomically
distinct CNS sites up to 230 days. Nature. PMID 36517603.
[AUTOPSY] - Rong Y, et al. (2024). Persistent spike in skull-meninges-brain axis.
Cell Host & Microbe. DOI.
[AUTOPSY + MECHANISTIC]
MMP-9 and blood-brain barrier:
- Kempuraj D, et al. (2024). SARS-CoV-2 spike stimulates microglia to
release MMP-9; MMP-9 degrades tight junction proteins. Int J Mol Sci.
PMID 39403255.
[PR]
Cognitive impairment in Long COVID:
- Hellmuth JM, et al. (2022). Risk factors and abnormal cerebrospinal fluid
associate with cognitive symptoms after mild COVID-19. Ann Clin Transl
Neurol 9(2):221-226. DOI;
PMID 35043593.
[PP]
Amyloid cross-seeding (biophysical):
- Wang H, et al. (2024). Spike fragments accelerate amyloid-beta
aggregation. Mol Neurobiol. DOI.
[AN] - Nyström S, et al. (2022). Spike promotes alpha-synuclein aggregation.
J Am Chem Soc. DOI.
[AN]
Hypothesis and sequence-level papers:
- Tetz G, Tetz V. (2022). SARS-CoV-2 prion-like domains and integrin-binding
motifs. Microorganisms. DOI.
[HYPOTHESIS] - Idrees D, Kumar V. (2021). SARS-CoV-2 spike and ACE2 amyloidogenic
regions. BBRC. DOI.
[AN]
SHED-conditioned medium (secretome composition):
- El Moshy S, et al. (2020). Dental stem cell-derived secretome/conditioned
medium: the future for regenerative therapeutic applications. Stem
Cells International 2020:7593402.
DOI;
PMID 32089709 /
PMC7013327.
[SR] - de Cara SPHM, et al. (2019). Angiogenic properties of dental pulp stem
cells conditioned medium on endothelial cells in vitro and in rodent
orthotopic dental pulp regeneration. Heliyon 5(12):e01560.
DOI.
[PR]
Edogawa clinical pathway (hospital-led programme):
- Edogawa Hospital DFPA + SHED programme. edogawadfpa.com.
Hospital-published pathway description; not a peer-reviewed outcomes paper.
[INV]
Additional supporting references cited for replication:
- Aksenova OV, et al. (2022). DOI.
- Cao Y, et al. (2023). DOI.
- Ma L, et al. (2022). DOI.
- Nahalka J. (2024). DOI.
- Petruk V, et al. (2020). DOI.
Investigator reports (not peer-reviewed):
- McCairn K. (2025). Cadaver Calamari: Amyloidogenic Fibrin Aggregates.
Substack.
[INV] - McCairn K. (2025). Amyloidogenic Fibrils in a Post-Gestational Case.
Substack.
[INV] - Perez J-C, Montagnier L. (2023). Cases of CJD following COVID-19
vaccination. IJVTPR. Link.
[HYPOTHESIS]
Commercial / media:
- Synaptek Labs blood sample protocol. Commercial; not independently validated.
Related Posts
- The Spikeopathy Research Cluster - the unifying clearance-and-tolerance framework this article connects to.
- Amyloid Pathology: SDF-1, Spike–Fibrin Interactions & Microclots.
- The Slow Burn, Part 1: Spike Persistence and Microclots.
- Methodology - how this article's evidence tags work.