Table of Contents
TL;DR: The Unseen Amyloid Burden
- A Mass Casualty Event: Neuroscientist Kevin McCairn, Ph.D., has publicly characterized the ongoing health crisis as a "Mass Casualty Event" (#MCE), driven by a novel amyloid pathology. (McCairn, 2025) [Investigator report; Needs replication]
- Novel Amyloid Fibrin: Forensic analysis of cadaveric and live blood samples reveals abnormal, rubbery, "calamari-like" fibrin aggregates that exhibit classic amyloid hallmarks: beta-sheet structure, fibrillar morphology, and resistance to fibrinolysis. (McCairn et al., 2025) [Investigator report; Needs replication]
- Gestational Transmission: Amyloidogenic fibrils have been identified in a 3-year-old child with in-utero exposure to mRNA vaccination, demonstrating the potential for long-term persistence and developmental impact. (McCairn, 2025) [Single case; Investigator report; Needs replication]
- A Crisis of Misdiagnosis: Standard blood tests (D-dimer, standard coagulation panels) are blind to these amyloid fibrin microclots. This creates a diagnostic void where patients with measurable organic pathology are told their symptoms are "anxiety," "post-viral fatigue," or "psychosomatic."
- The Spike Protein Engine: The SARS-CoV-2 spike protein, whether from infection or vaccination, has been shown to bind fibrinogen and induce this amyloidogenic transformation, creating persistent microclots that disrupt microcirculation and drive inflammation. (Nature, 2024; DOI: 10.1038/s41586-024-07873-4) [Peer-reviewed; Mechanistic in vitro / ex vivo with human readouts]
- Historical Warnings Ignored: The current crisis was foreshadowed by the late Prof. Luc Montagnier and others who warned of prion-like risks, with papers documenting sudden-onset Creutzfeldt-Jakob Disease following vaccination. (IJVTPR, 2023)
Introduction: The Pathology They Told You Didn't Exist
In Part 1, we detailed the "slow burn" of spike persistence, viral reactivation, and microclots. Now, we must confront the most severe and misunderstood consequence: a systemic amyloidogenic crisis.
While patients suffering from Long COVID and post-vaccination syndromes have been dismissed by a medical system relying on outdated diagnostics, a cohort of independent researchers has been documenting a clear, physical pathology. Led by the rigorous forensic work of neuroscientist Kevin McCairn, Ph.D., the evidence points to a mass-scale formation of amyloid fibrin aggregates—a pathology that explains the multi-system, chronic nature of these illnesses and reveals a terrifying gap in modern medicine's diagnostic capabilities.
This is not a rare condition. It is a widespread, undiagnosed burden. [Scope statement; prevalence estimates require population data]
Part 1: The McCairn Findings - From Cadavers to Children
The "Cadaver Calamari" Phenomenon
In a landmark preliminary report, McCairn and a team of researchers presented a forensic analysis of anomalous clots recovered from human cadavers. Their findings, which demand immediate replication and investigation, include:
- Gross Morphology: Unusual, rubbery, white, fibrous clots that are structurally distinct from typical thrombi. [Investigator report; Needs replication]
- Amyloid Hallmarks: The clots exhibited strong autofluorescence, Thioflavin T reactivity (indicating beta-sheet structure), and a dense, fibrillar ultrastructure under electron microscopy consistent with amyloid. [Investigator report; Needs standardized controls & blinded reads]
- Spike Protein Link: PCR analysis suggested the presence of molecular markers (SV40, Ori) associated with recombinant spike protein exposure. [Investigator report; Assay specificity/sensitivity must be independently verified]
The Conclusion: "These results may point to a novel or under-recognized pathology... a call for interdisciplinary scientific inquiry, clinical vigilance, and transparent investigation." - McCairn et al. [Investigator report]
The Living Proof: Amyloid in a Child
Perhaps the most alarming finding is the documented presence of amyloidogenic fibrils in the peripheral blood of a 3-year-old child with in-utero exposure to maternal mRNA vaccination. The child, who was born prematurely and required resuscitation, has suffered years of immune dysfunction.
- Fluorescence microscopy and SEM confirmed the presence of Thioflavin T-positive fibrils in the child's blood. [Investigator report; Single case; Needs replication]
- The fibrils showed striking morphological homology with the larger "calamari" clots found in cadavers. [Investigator report]
- This suggests the potential for long-term persistence of amyloidogenic fibrils seeded during gestation; cohort studies are required. [Single case inference; Needs cohort studies]
Part 2: The Mechanism - How Spike Creates an Amyloid Burden
The research provides a mechanistic link between spike exposure and this novel pathology:
- Spike-Fibrinogen Binding: The SARS-CoV-2 spike protein directly interacts with fibrinogen, the precursor to fibrin clots. (Nature, 2024) [Peer-reviewed; Mechanistic]
- Induction of Amyloid State: This interaction induces a conformational change in fibrin(ogen), pushing it into an amyloid state—a misfolded, resistant aggregate with a high beta-sheet content. (Grobbelaar et al., 2021) [Peer-reviewed; Mechanistic in vitro]
- Fibrinolysis Resistance: These amyloid fibrin clots are highly resistant to the body's natural clot-busting systems, allowing them to persist for months or years. (Pretorius et al., 2021-2022) [Peer-reviewed; Cohort/omics]
- Microvascular Occlusion: The persistent microclots lodge in capillaries, impairing oxygen delivery to tissues (ischemia) and causing a cascade of inflammatory and oxidative damage. [Biological plausibility; Human correlation under study]
Replication To-Do: blinded inter-lab thromboelastography/fluorescence protocols, predefined thresholds, ring trials; correlate with tissue oxygen extraction and symptom severity.
Part 3: The Mass Misdiagnosis - "It's All in Your Head"
This is the central crisis. Patients are presenting with a clear, organic pathology, but our standard medical toolkit is blind to it.
Why Patients Are Being Misdiagnosed:
| Patient’s reality | Conventional response | The flaw |
|---|---|---|
| Debilitating fatigue, brain fog, myalgia | “Labs are normal—likely anxiety/depression/post-viral.” | CBC/chemistry and D-dimer don’t detect amyloid-like fibrin microclots. |
| Palpitations, chest pain, dyspnea | “EKG/troponin negative—unlikely cardiac.” | Microvascular ischemia can evade standard cardiac tests. |
| Paresthesias, word-finding issues | “MRI clear—no neurological cause.” | Microcirculatory impairment can precede structural MRI changes. |
The consequence is a large population of individuals being labeled with functional disorders or dismissed, while a measurable physical pathology may go unaddressed. Diagnostic development needed
Part 4: The Neurological and Prion-Like Threat
The amyloid nature of these clots raises a terrifying specter: prion-like disease.
- Prion-Like Propagation: Amyloid fibrils can act as seeds, templating the misfolding of native proteins in a self-propagating cascade. This is the core mechanism of prion diseases like CJD.
- Montagnier's Final Warning: The late Nobel laureate Prof. Luc Montagnier's last paper, in peer review at his death, detailed 26 cases of Creutzfeldt-Jakob Disease with symptoms appearing an average of 11.38 days after a COVID-19 injection. (IJVTPR, 2023)
- Synergistic with Neurodegeneration: The presence of systemic amyloid fibrin could exacerbate or accelerate underlying neurodegenerative processes, particularly in genetically susceptible individuals (e.g., APOE4 carriers).
Prion-like seeding is biophysically plausible for amyloids in general; population-level prion disease attribution here is not established and would require rigorous case definitions, neuropathology, and controls.
A Call for a New Diagnostic Paradigm
The work of McCairn and others is not just an academic exercise. It is a roadmap for saving lives.
- Acknowledge the Pathology: The medical and public health establishment must officially recognize amyloid fibrin microclots as a legitimate pathological entity in Long COVID and post-vaccination syndromes. [Position]
- Implement Available Diagnostics: Protocols for detecting amyloid microclots in live blood, using fluorescence microscopy and specialized staining, exist and must be made accessible. (Synaptek Labs Protocol) [Investigator protocol; Requires validation]
- Stop the Misdiagnosis: Physicians must be educated that patients with these symptom profiles likely have an organic, measurable condition, even if standard tests are normal. [Position]
- Urgently Research Treatments: The focus must shift to finding ways to safely dissolve these resistant clots and clear the amyloid burden, exploring therapies like fibrinolytic agents, plasmapheresis, and other novel approaches. * Not medical advice *
Standardization Priorities: assay controls, blinded image review, inter-rater reliability, longitudinal follow-up, and linkage to functional outcomes.
Key Resources & Evidence
Primary McCairn Publications
- Cadaver "Calamari" Amyloidogenic Fibrin Aggregates - Full forensic report [Investigator report]
- Amyloidogenic Fibrils in a Post-Gestational Case - Child case study [Investigator report; Single case]
- Warning: Global amyloidogenic health disaster - Video presentation [Media]
Images with captions / alt text:
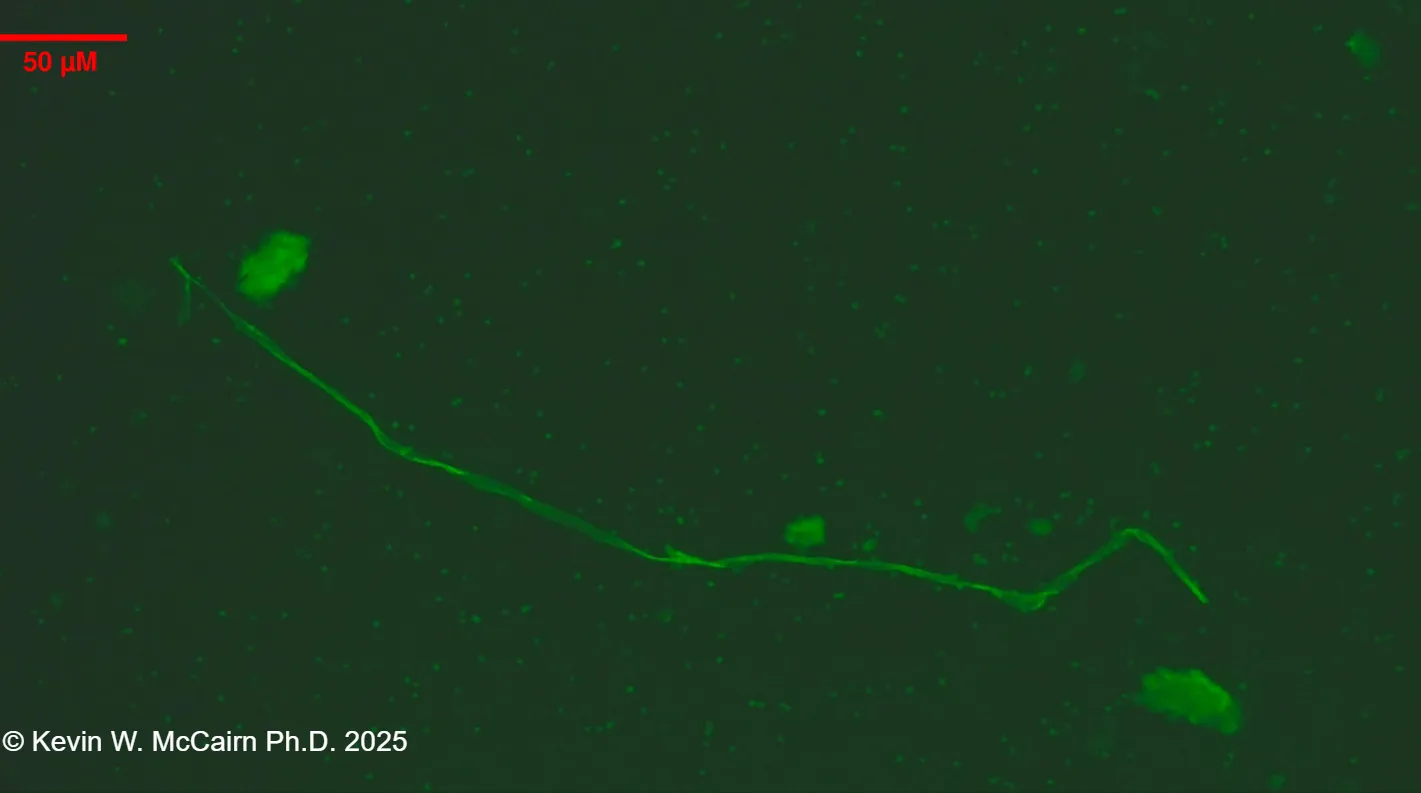
Caption: Representative image from Slide 18 (UV ThT fluorescence). Alt: UV ThT fluorescence micrograph showing amyloid-like fibrils.
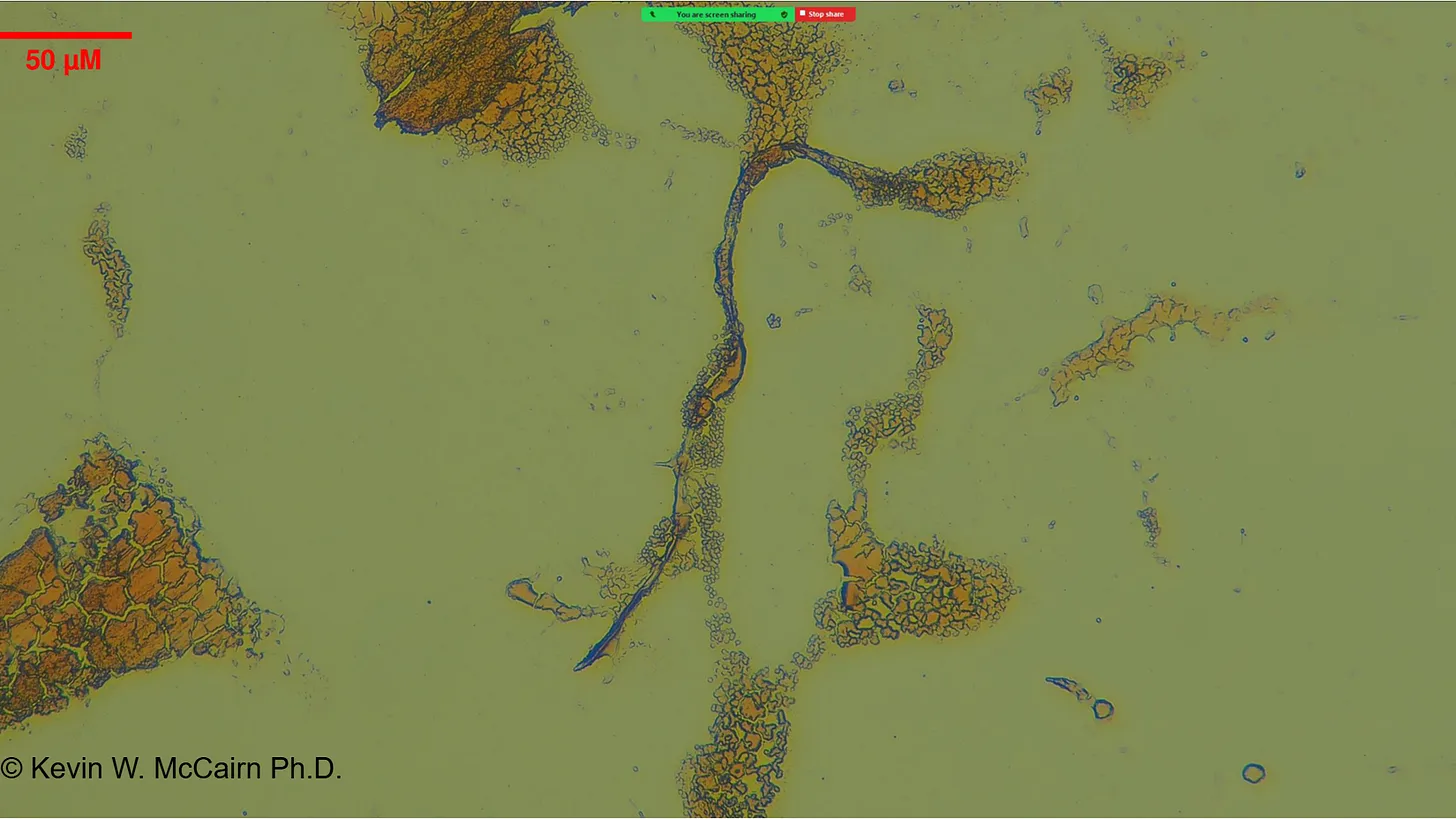
Caption: Representative light-microscopy micrograph (Slide 3). Alt: Light microscopy image showing fibrillar structures.
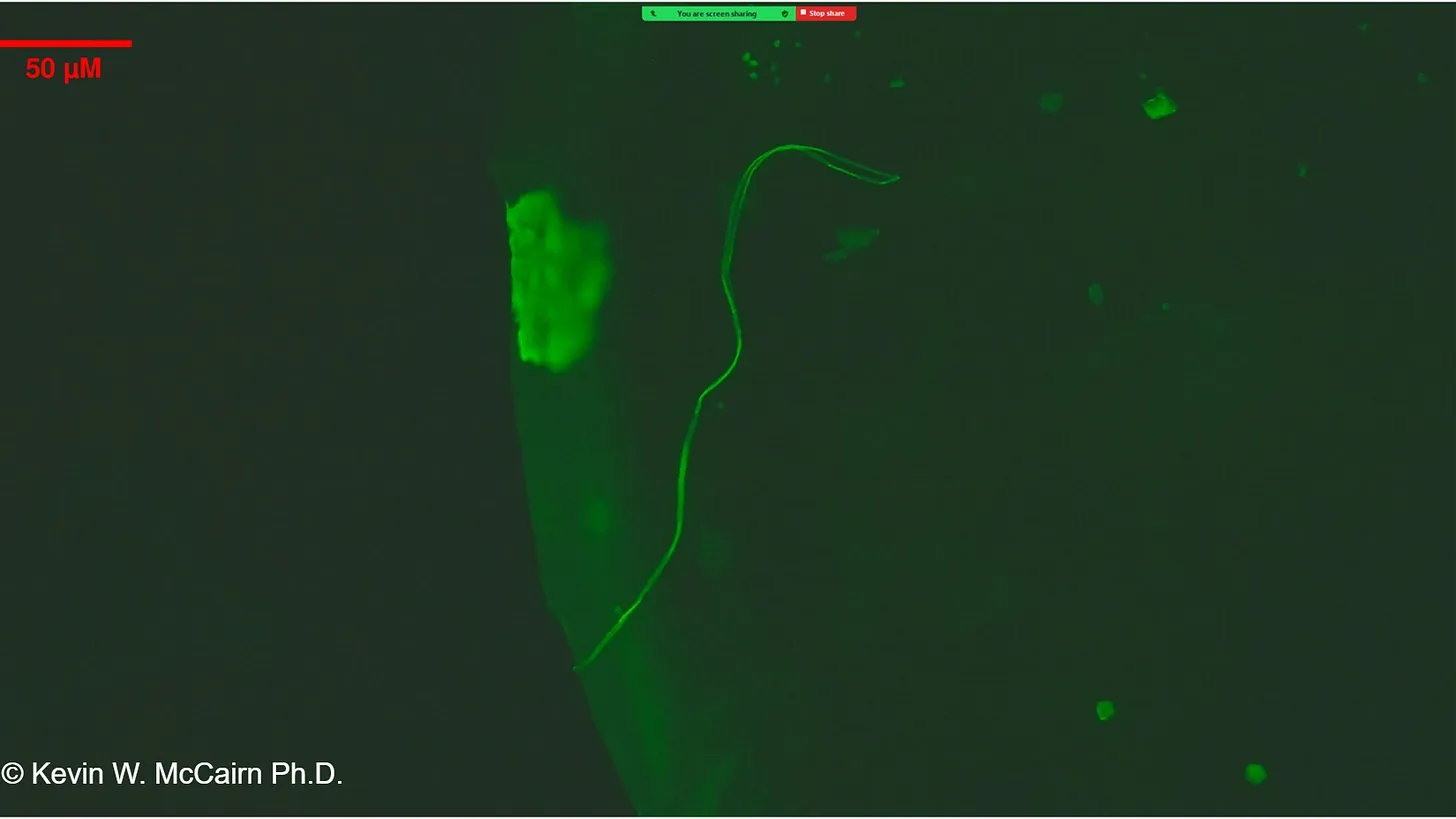
Caption: Thioflavin T micrographs showing amyloid-like fibrils in peripheral blood. Alt: Fluorescence micrograph of Thioflavin T–positive fibrils.
Supporting Research
- Spike protein induces fibrin amyloid microclots - Grobbelaar et al. 2021 [Peer-reviewed; Mechanistic in vitro]
- Long COVID microclots & proteomics - Pretorius et al. 2021-2022 [Peer-reviewed; Cohort/omics]
- Fibrin drives thromboinflammation - Nature 2024 [Peer-reviewed]
- CJD cases post-COVID vaccination - Montagnier et al. 2023
Diagnostic Resources
- Synaptek Labs Blood Sample Protocol [Investigator protocol]
- The Ethical Skeptic: Houston We Have Another Problem
Amyloid Formation and Neurodegeneration
Multiple recent studies link the SARS‑CoV‑2 spike protein (and fragments thereof) to amyloidogenic processes that are relevant to neurodegeneration. The literature includes biochemical, cellular, and animal-model evidence showing that spike-derived peptides can form or accelerate amyloid-like aggregates and that spike can persist in or traffic to CNS-associated compartments in some cases. Below is a concise summary with peer-reviewed citations and DOIs for direct reference.
Spike protein and amyloidogenesis
Evidence from biophysical and cellular studies indicates that spike fragments—including portions of the receptor-binding domain (RBD)—can adopt beta‑sheet–rich conformations and form fibrils in vitro, and that they can accelerate aggregation of endogenous amyloidogenic proteins under experimental conditions.
- Wang et al. (2024), Spike fragments accelerate amyloid‑beta aggregation (Alzheimer’s connection). DOI: https://doi.org/10.1007/s12035-023-03726-9
- Nyström et al. (2022), Spike promotes α‑synuclein aggregation (Parkinson’s link). DOI: https://doi.org/10.1021/jacs.2c03925
Spike detection in brain-associated compartments
Several studies report detection of spike protein or spike-derived peptides in brain tissue or meningeal compartments after infection or exposure in limited cohorts or models. These observations motivate additional work on routes of access and the functional consequences of persistent protein fragments.
- Rong et al. (2024), Persistent spike in brain tissue along skull/meninges axis; DOI: https://doi.org/10.1016/j.chom.2024.11.007
Sequence motifs, inserts, and engineering hypotheses
Sequence-level analyses have called attention to short inserts and motif similarities between spike and other proteins; some authors have noted gp120-like motifs and other similarities. Such observations are hypothesis‑generating; they require careful evolutionary and biochemical follow-up before being used to draw mechanistic or intent-related conclusions.
- Tetz & Tetz (2022), motif and insert analysis; DOI: https://doi.org/10.3390/microorganisms10020280
Gene‑delivery and genomic safety discussions
Theoretical concerns have been raised about interactions between delivery platforms (self‑amplifying RNA, viral vectors, and CRISPR/Cas systems) and host genomes, including off‑target editing risks tied to PAM motifs or integration. These are active areas of safety research; demonstration of a risk requires compatible enzymology, delivery, and validated off‑target activity in vivo.
Additional studies and resources
Further references provided for the curious reader and for replication/verification efforts:
- Aksenova et al. (2022): https://doi.org/10.3390/ijms232113502
- Cao et al. (2023): https://doi.org/10.1021/acsami.3c09815
- Idrees & Kumar (2021): https://doi.org/10.1016/j.bbrc.2021.03.100
- Ma et al. (2022): https://doi.org/10.1038/s41421-022-00458-3
- Nahalka (2024): https://doi.org/10.3390/ijms25084440
- Petruk et al. (2020): https://doi.org/10.1093/jmcb/mjaa067
- Interview with Dr. Kevin McCairn (media): https://rumble.com/v6sd87z-warning-global-amyloidogenic-health-disaster-with-dr-kevin-mccairn.html
Limitations & Open Questions
Non-random sampling; selection bias possible.
Lack of multi-site, blinded replication for several investigator reports.
Assay specificity/sensitivity and thresholds need standardization.

